-
(786) 502-2173
-
We've gone mobile!
-
Hours: By Appointment Only
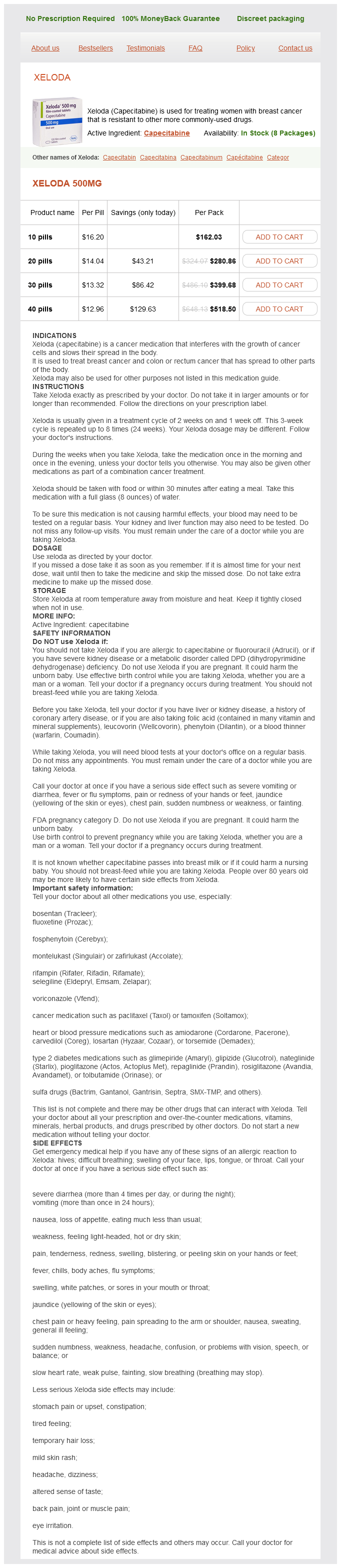
Only $12.96 per item
Xeloda dosages: 500 mg, 500 mg
Xeloda packs: 10 pills, 20 pills, 30 pills, 40 pills
In stock: 505
If the patient has moderately symptomatic hyponatremia menopause palpitations discount 500 mg xeloda free shipping, the best initial therapy is a limited trial infusion of isotonic saline to see if the serum [Na+] improves (1). Is measurement of urine sodium concentration valid in patients who have already received saline administration prior to consultation Should a trial of fluid restriction be performed if the patient manifests predictors of failure of fluid restriction The predictors of failure of fluid restriction (Table 413) indicate the relative likelihood of failure of fluid restriction, but not an absolute certainty. However, if fluid restriction is attempted in the presence of one or more of these predictors, the stringency should be increased to have the best chance of success. Liver function abnormalities in patients receiving vaptans occurred in clinical trials of polycystic kidney disease using 35 times the dose of tolvaptan recommended for the treatment of hyponatremia for >3 months (1). As in the previous question, the recommendation that tolvaptan not be used for >30 d is based on the occurrence of liver failure in a small number of patients treated with higher doses. Therefore, the decision of how long to treat a patient should be based on a clinical determination of risk versus benefit for individual patients. However, if tolvaptan is prescribed for periods longer than 30 d, it is appropriate to monitor liver function tests every 3 months at least during the first year of therapy (1). Hyponatremia, cerebral edema, and noncardiogenic pulmonary edema in marathon runners. Study of brain electrolytes and organic osmolytes during correction of chronic hyponatremia: implications for the pathogenesis of central pontine myelinolysis. Rapid correction of hyponatremia produces differential effects on brain osmolyte and electrolyte reaccumulation in rats. Hyponatremia: a prospective analysis of its epidemiology and the pathogenetic role of vasopressin. Hyponatremia improvement is associated with a reduced risk of mortality: evidence from a meta-analysis. Hyponatremia, convulsions, respiratory arrest, and permanent brain damage after elective surgery in healthy women. Statement of the Second International Exercise-Associated Hyponatremia Consensus Development Conference, New Zealand, 2007. Neurologic sequelae after treatment of severe hyponatremia: a multicenter perspective. A syndrome of renal sodium Emergency Management of Acute and Chronic Hyponatremia loss and hyponatremia probably resulting from inappropriate secretion of antidiuretic hormone. Postoperative hyponatremia despite near-isotonic saline infusion: a phenomenon of desalination [see comments]. Assessment of the efficacy and safety of intravenous conivaptan in euvolemic and hypervolemic hyponatremia. Treatment of the syndrome of inappropriate secretion of antidiuretic hormone with urea in critically ill patients.
Elderberry. Xeloda.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96444
False positive results can be caused by catecholamine-containing foods (coffee womens health youngkin order 500 mg xeloda with amex, processed meat, fermented foods), certain antipsychotics, selective -adrenergic blockers, and -adrenergic receptor blockers (44). Alpha-adrenergic blockers that antagonize catecholaminestimulated vasoconstriction are the agents of choice. A recommended perioperative management protocol of pheochromocytomas has been described (44). Approximately 35% of cases are associated with germ line or somatic mutations (45). Physical examination along with personal and family history may elucidate clues to inherited disorders. The physical finds of caf´ -au-lait spots and e neurofibromas suggest Neurofibromatosis Type 1. Hyperthyroidism Thyroid storm is an exaggerated manifestation of hyperthyroidism or thyrotoxicosis. An inciting event such as surgery, infection or the administration of iodinated contrast dyes, iodine or lithium precipitates thyroid storm (46). Thyrotoxic periodic paralysis is a rare complication of thyrotoxicosis that can be potentially fatal when there is weakness of the respiratory muscles and cardiac arrhythmias due to hypokalemia. This condition is most common in young adult males (2040 years of age) of Asian descent (47). Propylthiouracil at a loading dose of 500 1000 mg followed by 250 mg every 4 hours or methimazole (carbimazole) at a daily dose of 6080 mg is recommended to inhibit new synthesis of thyroid hormones in thyroid storm (48). In addition to inhibiting thyroid hormone production, propylthiouracil inhibits the conversion of T4 to T3. Glucocorticoids also inhibit peripheral conversion of T4 to T3 and can be used as an adjunct therapy. Growth Hormone Excess Growth hormone excess causes gigantism while the epiphyseal growth plates are open during childhood. In adolescence and young adulthood in which the growth plates are closed, this disorder leads to acromegaly and coarsening of the facial features. Treatment options for pituitary gigantism include surgery, radiation, and medical therapy (octreotide, bromocriptine, pegvisomant) based on circumstances and availability (49). Management Evaluation to determine the etiology of hypertension should occur concurrently and not delay treatment of hypertension. In the setting of less severe elevations, oral agents can be considered for initial management. In a prospective study of 31 children and adolescents, three children had transient water imbalance, 8 had hyperprolactinemia, and 1 had adrenal insufficiency but all resolved. Sperling to ensure early detection of hormonal deficiencies should be performed starting 1 year after injury. Fluid resuscitation should be initiated with the aim of lowering serum sodium slowly to avoid osmotic demyelination syndrome. This condition typically occurs in patients with undiagnosed chronic hypothyroidism presenting with an acute systemic illness.
The authors strongly recommend deferring treatment of anatomic lesions until the end of the entire lysis procedure to avoid this risk pregnancy 8 weeks heartbeat buy xeloda 500 mg fast delivery. For example, dilating a MayThurner lesion on the first day of treatment, before thrombus clearance, is a critical mistake to be avoided. Frequent puncture site checks for bleeding/hematoma are crucial, with avoidance of all intramuscular/intra-arterial injections/punctures. Simultaneous heparin (or argatroban monohydrate) infusions through the access sheath(s) must be used to prevent the opened venous segment from immediately reoccluding. Additional laboratory testing includes hemoglobin, prothrombin time, and platelet count, which will reveal any ongoing bleeding or risk thereof. Ideally, the lytic agent infusion should be reduced, not stopped, while correction and laboratory retesting occurs. Red cell transfusion should be considered if hemoglobin falls below 8 mg/ dL or anemia is symptomatic. The authors cannot stress enough that any correction must be timely and aggressive. Patients are maintained on bed rest for 2 hours and then allowed to ambulate with assistance as needed. Clinical and sonographic evaluation is performed at follow-up visits 1, 6, and 12 months after the procedure. Anticoagulation is maintained for a minimum of 36 months following thrombolysis in uncomplicated cases, with longer treatment regimens for those with a presumed hypercoagulable state. Most bleeding is easily managed, although it may require cessation of the lysis procedure. If significant bleeding occurs, the lytic agent should be stopped and hemostasis should be the goal with manual compression or sheath upsizing if at the access site. In consultation with the Hematology Department, oral anticoagulation was discontinued after 1 year. Contrast injection shows an area of stenosis (arrow, b) in the proximal left common iliac vein, with multiple filling defects extending to the caval junction. Images showing appropriate stent position with excellent opacification of the left iliac vein. Post-thrombotic syndrome after catheter-directed thrombolysis for deep vein thrombosis (CaVenT): 5-year follow-up results of an open-label, randomised controlled trial. Determinants of early and long-term efficacy of catheter-directed thrombolysis in proximal deep vein thrombosis. After obtaining informed consent, the patient is placed supine on the procedure table, which is positioned in reverse Trendelenburg to distend the veins in the lower extremities. For veins <2 mm, nitroglycerine paste may be applied to the primary insertion site to dilate the vein and prevent venospasm before gaining intravascular access. Hemoglobin absorption does not play a role when using a wavelength >1320 nm, and water absorption is the dominant mechanism. The choice of thermal ablation mechanism depends on the operator and patient preference.
Syndromes
Additional information:
Usage: p.c.
Tags: buy cheap xeloda 500 mg on line, cheap 500 mg xeloda overnight delivery, discount xeloda 500 mg otc, 500 mg xeloda order otc
Angir, 46 years: Injury to the ramus mandibularis (mandibular nerve) can occur if dissection is done too close to the angle of the mandible, resulting in flattening of the lower lip. Taste and olfactory changes following laparoscopic gastric bypass and sleeve Michael A. Other autogenous options include: (1) radial branchcephalic direct access (snuffbox fistula) (2) ulnarbasilic forearm transposition; (3) brachialcephalic upper arm direct access (antecubital vein to brachial artery); and (4) brachialbasilic upper arm transposition (basilic vein transposition). Pheochromocytoma multisystem crisis successfully treated by emergency surgery: report of a case.
Irmak, 29 years: Use of clevidipine for intraoperative hypertension caused by an undiagnosed pheochromocytoma: a case report. Society of hospital medicine glycemic control task force summary: practical recommendations for assessing the impact of glycemic control efforts. A roll is positioned under the right axilla and the air is evacuated from the beanbag. Having completed dissection, the artery is palpated and assessed to ensure that it can be successfully clamped and oversewn, while still leaving adequate length for transposition to the carotid artery.
Angar, 27 years: Seven years of treatment with risedronate in women with postmenopausal osteoporosis. This allows precise anatomic evaluation, and repeated magnified and oblique views of any regions of interest, while minimizing contrast. In patients with better hemodynamic stability, proximal control at the pararenal level, as previously described, is usually preferred. It is important to image not only the aortic arch, but also the outflow, including the entire cervical and intracranial vasculature.
Olivier, 42 years: When endocrine emergencies arise in this often critically ill and complex population, there are unique clinical factors that must be considered. Proximally, care should be taken to minimize unnecessary dissection, which can cause autonomic sexual dysfunction in male patients if pelvic splanchnic nerves are transected. Typically, if one target vessel is offset (usually in a cranial/caudal position), all the target vessels will be shifted similarly. If there is no Doppler signal after these steps, one must consider Open management of the popliteal artery Injuries to the popliteal vessels can be quite challenging.
Innostian, 60 years: Primary adrenal insufficiency caused by adrenalitis associated with cytomegalovirus infections has been reported in patients with immunodeficiency, including after transplantation (26). Electrocardiogram changes or arrhythmias intraoperatively or postoperatively should prompt a cardiology consultation. It should be noted that hunger, per se, is a poor symptom discriminator for hypoglycemia. Rarely, long-standing tracheomalacia may cause collapse of the tracheal wall with airway obstruction.