-
(786) 502-2173
-
We've gone mobile!
-
Hours: By Appointment Only
Only $2.26 per item
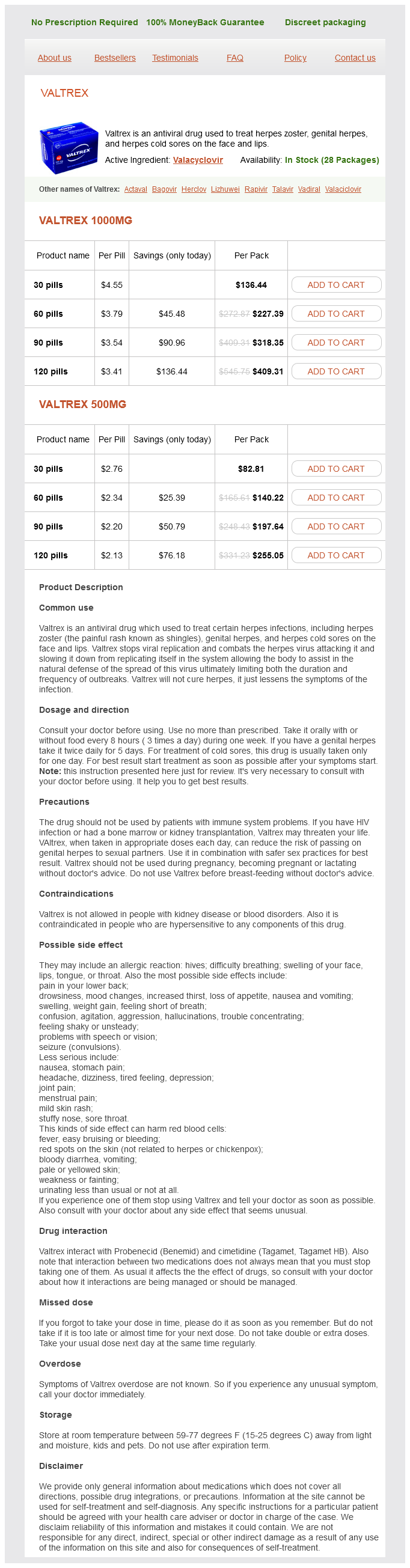
Valtrex dosages: 1000 mg, 500 mg
Valtrex packs: 30 pills, 60 pills, 90 pills, 120 pills
In stock: 999
An inactivated vaccine is available for travellers spending time in endemic areas anti viral apps valtrex 500 mg buy online. Clinical features Many of these infections cause a mild self-limiting illness with fever, headache and drowsiness. If the patient is in a coma, the prognosis is poor, whether or not treatment is given. Brain and spinal abscesses An intracranial abscess may develop in the epidural, subdural or intracerebral sites. Epidural abscesses are uncommon; subdural abscess presents similarly to intracerebral abscess. Cerebral abscess Infection follows the direct spread of organisms from a parameningeal infective focus. Infection with tubercle bacilli may result in chronic caseating granulomata (tuberculomas) presenting as intracranial mass lesions. Clinical features these include headache, focal neurological signs, seizures and sometimes evidence of raised intracranial pressure (p. Lumbar puncture is not performed because of the danger of coning in the presence of raised intracranial pressure (p. Management Treatment is with a combination of intravenous antibiotics and sometimes surgical decompression. Spinal epidural abscess Back pain and fever are followed by paraparesis and/or root lesions. Encephalitis and brain abscess Toxoplasma, cytomegalovirus, herpes simplex and other organisms cause severe encephalitis. Primary intracranial tumours are derived from the skull itself, or from any of the structures lying within it, or from their tissue precursors. They may be malignant on histological investigation but rarely metastasize outside the brain. Clinical features the clinical features of a cerebral tumour are the result of the following: Progressive focal neurological deficit Raised intracranial pressure Focal or generalized epilepsy. Neurological deficit is the result of a mass effect of the tumour and surrounding cerebral oedema. Subsequent involvement of the frontal speech area and motor cortex produces expressive aphasia and hemiparesis. Parietal lobe tumours cause a homonymous field defect, cortical sensory loss, hemiparesis and partial seizures on the side contralateral to the tumour. Rapidly growing tumours destroy cerebral tissue and loss of function is an early feature. The headache typically changes with posture and is made worse by coughing, sneezing, bending and straining. As the tumour grows there is downward displacement of the brain and pressure on the brainstem, causing drowsiness, which progresses eventually to respiratory depression, bradycardia, coma and death.
Pomegranate Leaf Extract (Pomegranate). Valtrex.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96406
The patient is placed supine on the operating table and the head supported with a head ring hiv infection rash valtrex 1000 mg buy. A decongestant or topical anaesthetic with adrenaline is applied to the nose, usually in the anaesthetic room. A 0° Hopkins rod with an appropriate light source is passed into the nasal cavity, and the nasopharynx is carefully examined. The fossa of Rosenmüller in particular must be assessed, as this may harbour a malignancy. Biopsies are taken, if indicated, with straight BlakesleyWilde or TilleyHenckel forceps. Adrenaline-soaked neuropatties or diathermy can be applied if required for haemostasis. Otitis media with effusion secondary to inadvertent damage to the Eustachian tube orifice. In many cases the proximal trachea can be assessed, as described in Chapter 24, with a laryngoscope and a 0° Hopkins rod. Selection of an appropriately sized bronchoscope is essential for paediatric patients. Appropriate optical forceps must be available if foreign body removal is required. Safe bronchoscopy requires good teamwork and communication between the surgeon and the anaesthetist. When the patient is well oxygenated and the anaesthetist feels it is appropriate, the endotracheal tube or laryngeal mask is withdrawn and a mouth guard placed over the upper teeth. Using the anaesthetic laryngoscope, the larynx is visualized as the non-dominant hand supports the laryngoscope. The bronchoscope is held in the dominant hand and advanced until the larynx is reached. The bronchoscope may be rotated through 90° to facilitate passage through the glottic opening, which minimizes the risk damage to the vocal cord from the tip of the bronchoscope. Once the bronchoscope is in the proximal trachea, the anaesthetic circuit is connected and the bronchoscope is advanced towards the carina. By gently turning the head to the left, the bronchoscope can be advanced into the right main bronchus, and vice versa. Secretions can be removed using narrow suction tubing, which can be advanced by an assistant or scrub nurse. If a foreign body, especially an organic foreign body is visualized, it is vital that a small volume of 1:10,000 adrenaline is instilled via the suction tubing to reduce mucosal oedema and to allow vasoconstriction. This improves access and minimizes the risk of bleeding which can make removal of the foreign body very challenging.
Aortic regurgitation: clinical hiv throat infection symptoms cheap valtrex 500 mg buy online, hemodynamic, surgical, and angiographic correlations. Diagnosis of aortic insufficiency: comparison of auscultation and M-mode echocardiography to angiography. Detection of aortic insufficiency by standard echocardiography, pulsed Doppler echocardiography, and auscultation: a comparison of accuracies. The Graham Steell murmur versus aortic regurgitation in rheumatic heart disease: results of aortic valvulography. Pathophysiologic determinants of third heart sounds: a prospective clinical and Doppler echocardiography study. Hills sign in aortic regurgitation: enhanced pressure wave transmission or artefact Clinical significance and hemodynamic correlates of the third heart sound gallop in aortic regurgitation: a guide to optimal timing of cardiac catheterization. Premature mitral valve closure: a hemodynamic explanation for absence of the first sound in aortic insufficiency. The Austin Flint murmur: its differentiation from the murmur of rheumatic mitral stenosis. The intensity of the murmur behaves in distinctive ways during maneuvers, altering venous return to the heart (see Chapter 43). Although pulsus bisferiens has been described in hypertrophic cardiomyopathy,2 this refers to a finding seen on intra-arterial pressure tracings, not a palpable one at the bedside. Associated cardiac findings are an enlarged, laterally displaced palpable apical movement,7 a palpable lower parasternal movement from an enlarged left atrium or associated tricuspid regurgitation (see Chapter 38),8 and in younger patients a hyperkinetic arterial pulse (see Chapter 15). Because of their low ejection fraction, these patients often do not tolerate valve replacement. The degree of this movement correlates well with severity of regurgitation (r = 0. The physical signs of acute and chronic mitral regurgitation differ in several ways. In acute lesions, patients are acutely ill with elevated neck veins and signs of pulmonary edema; in chronic lesions, these signs may be absent. In acute lesions the fourth heart sound is common (80% in one series); in chronic lesions the fourth heart sound is rare, either because the atrial contraction is absent. The murmur, which is usually transient, may be holosystolic, midsystolic, or late systolic. It appears in up to 20% of patients with myocardial infarction,22 in whom it is associated with a higher incidence of persistent chest pain in the intensive care unit (45% vs. It is an important cause of late systolic murmurs and mid-to-late systolic clicks,23-25 and in developed nations it is the most common cause of mitral regurgitation. It is characteristically late systolic because the mitral leaflets are well supported by chordae tendineae and competent during early systole, but lose this support as the ventricle becomes smaller during late systole, allowing the leaflets to buckle backward toward the left atrium and create a regurgitant leak.
Syndromes
Additional information:
Usage: p.r.n.
Tags: cheap valtrex 500 mg buy line, cheap valtrex 500 mg free shipping, valtrex 500 mg purchase mastercard, order valtrex 500 mg otc
Kurt, 28 years: In addition to the incision in the mastoid skin, I employ a transverse counter incision, typically located midway along the vertical axis of the flap, to facilitate dissection and elevation of the flap.
Silas, 62 years: Proteins (called apoproteins) embedded into the phospholipid coating exert a stabilizing function and allow the particles to be recognized by receptors in the liver and peripheral tissues.
Xardas, 36 years: There are, however, significant disadvantages to bilobed flap reconstruction, including complex incision lines that are, by definition, impossible to be placed within relaxed skin tension lines.
Kalesch, 54 years: Cutting and suture technique of the caudal septal cartilage for the management of caudal septal deviation.
Sanford, 26 years: Group 3: Humerus structures; radius and ulna markings; carpals, metacarpals, and phalanges.
Kafa, 30 years: Wood and Wolferth first described trepopnea in patients with congestive heart failure.
Brontobb, 52 years: Reliability refers to how often multiple clinicians, examining the same patients, agree that a particular physical sign is present or absent.