-
(786) 502-2173
-
We've gone mobile!
-
Hours: By Appointment Only
Only $1.56 per item
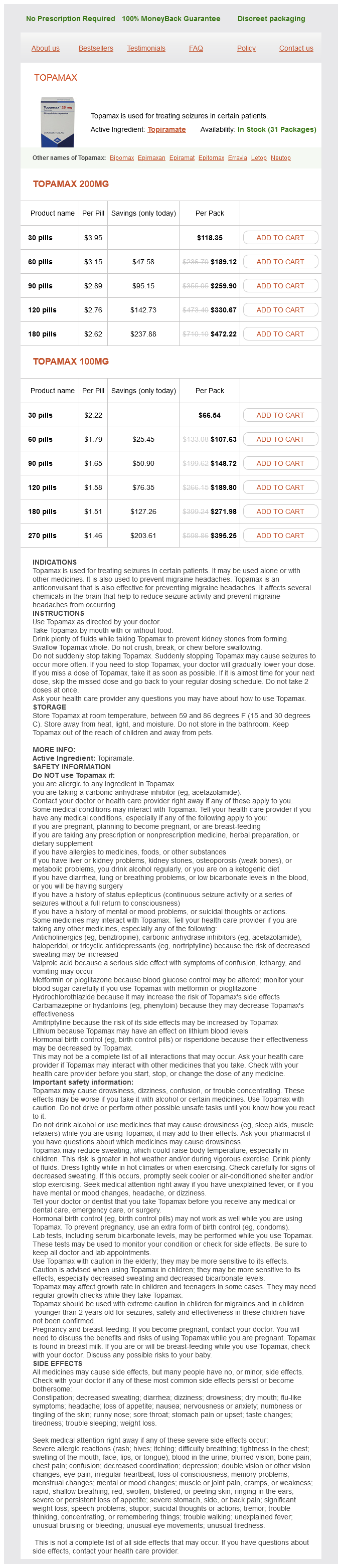
Topamax dosages: 200 mg, 100 mg
Topamax packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills
In stock: 589
These correlations suggested that patients with moderate hematomas might be candidates for a controlled clinical comparison of surgical and conservative treatment medicine omeprazole 20mg topamax 200 mg buy low cost. Mortality rates for lobar hemorrhages at these volumes were 7%, 60%, and 71%, respectively. In contrast, of the 91 patients who survived with hematoma volumes of less than 30 cm3, 16 (18%) were independent. Patients who were younger than 59, 60 to 69 and older than 70 years had 59%, 33%, and 17% good or excellent outcomes, respectively. All patients with hematoma volumes greater than 85 cm3 died, irrespective of treatment, and all patients with hematoma volumes of less than 26 cm3 survived without surgery. For large hematomas (>50 cm3), there was no difference in functional outcome between the two groups, but the mortality rate was lower in the surgical group than in the conservative group (48% versus 90%). This study suggests that surgical evacuation may play a lifesaving role in patients with large hematomas by sparing viable local brain function by decreasing mass effect, progressive edema, or impaired cerebral perfusion. The overall lower surgical mortality rate (30%) in this study in comparison to others may reflect surgical technique and is discussed later in this chapter. Large-volume thalamic hematomas are more devastating than similarly sized subcortical or putaminal hematomas. This was seen when the scans were obtained early; none of the patients showed an increase in hematoma size after 24 hours. On the 1-hour follow-up scan, 26% of patients exhibited hematoma growth (>33% enlargement). Therefore, 38% of the patients exhibited hematoma progression within 24 hours of hemorrhage. Of these patients, 33% deteriorated within the first hour, and an additional 25% deteriorated within the next 20 hours. This finding implies that early hematoma evacuation may not only reduce perihematomal ischemia160,196,197 and the toxic effect of blood products160,200,201 but also contain potential hemorrhagic progression. In this study, the most important risk factor for progression was persistent hypertension. The goals of surgical evacuation of a hematoma are to reduce the mass effect, block the release of neuropathic products from the hematoma, and prevent prolonged interaction between the hematoma and normal tissue, which can initiate pathologic processes. Surgical removal of the clot may improve the function and recovery in this penumbra. Removing these patients from the analysis plus focusing on superficial hematomas presents a better picture for surgery. When the prognosis-based Rankin score was used as the outcome variable, a significant benefit was observed for surgical patients in this subgroup (P =.
Glossy Buckthorn (Alder Buckthorn). Topamax.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96823
Despite the risk for intracerebral hemorrhage, the benefit of using systemic heparin was examined in a large retrospective study by Ameri and Bousser treatments yeast infections pregnant topamax 200 mg purchase on-line. If an infectious process is identified, broad-spectrum antibiotics or drainage of purulent collections should be part of the treatment. Increased intracranial pressure can be treated with osmotic agents (mannitol, hypertonic saline), temporary shortterm hyperventilation, drainage of cerebrospinal fluid by ventriculostomy or lumbar puncture, barbiturate coma, or surgical craniectomy. The patient progressed from being unresponsive initially to having just mild dysphasia at 4 weeks. Barnwell and coworkers reported direct transjugular endovascular thrombolytic therapy in three patients. In two patients, the clinical signs and symptoms improved, with angiographic evidence of clot lysis and dural sinus recanalization. Angiography indicated that one patient had partial resolution of a clot in the torcular Herophili and transverse sinus, but that patient showed no clinical improvement. These preliminary results were encouraging and suggested that transjugular local infusion of thrombolytic agents can be an effective and safe treatment of symptomatic, thrombosed dural sinuses. Tsai and colleagues reported five cases of successful direct transfemoral thrombolytic treatment. Patency of the affected dural sinus was achieved along with antegrade flow in all patients. Six patients either improved neurologically over their prethrombolysis state or were healthy after thrombolysis. The only complications were an infected femoral access site and transient hematuria. Contraindications to thrombolytic therapy include recent childbirth, history of a bleeding diathesis, recent major surgery, recent major trauma, active gastrointestinal bleeding, or inflammatory bowel disease. It has been suggested that local infusion of thrombolytic agents via interventional neuroradiologic techniques can minimize the side effects seen with systemic thrombolytic therapy. Follow-up imaging demonstrated significant sinus recanalization, and the patient was left with just minor neurological deficits. Local infusion of thrombolytics offers advantages, including minimization of systemic effects and local clot lysis with high concentrations of thrombolytic agents (Tables 357-1 and 357-2). Routes of access include the transfemoral and transjugular routes, as well as direct puncture of the dural sinuses. Historically, Scott and colleagues reported the first use of local fibrinolytic therapy. Barnwell and colleagues reported an additional six cases of local thrombolytic therapy.
Although the value of environmental interventions is widely recognized, they remain substantially underutilized (59) symptoms 1974 buy topamax 200 mg online. Structure and support for the patient Nursing, psychological, general medical, and psychiatric staff and family members can also provide cognitive-emotional support designed to strengthen any retained adaptive cognitive functioning that the patient possesses. The goal of these interventions is to reduce anxiety and the unfamiliar while providing understanding and support. Central to providing cognitive and emotional support are efforts to deal with disorientation. All who come in contact with the patient should provide reorientation, which entails reminding the patient in an unpressured manner of where he or she is, the date and time, and what is happening to him or her. The patient should be told that the symptoms are temporary and reversible and do not reflect a persistent psychiatric disorder. Similarly, the perception of cognitive deficits may lead patients to conclude that they have suffered brain damage. Unless the delirium is thought to be due to a major stroke or injury or to another event that may cause permanent brain injury, all who have contact with the patient should reassure her or him that these deficits are common and reversible symptoms associated with the particular illness, surgery, or other treatment. There have been no large clinical trials examining the efficacy of cognitive and emotional support in delirium. However, as with environmental interventions, increased use of these currently underutilized supportive measures has been encouraged on the basis of clinical experience, common sense, and lack of adverse effects (59). Treatment of Patients With Delirium 21 Copyright 2010, American Psychiatric Association. The high-potency antipsychotic medication haloperidol is most frequently employed, although other pharmacologic and somatic interventions have been used in particular instances. The available studies of the efficacy and other outcomes from use of these treatments for patients with delirium are reviewed in this section. Several important points should be considered when evaluating the evidence for specific somatic interventions. While haloperidol has been the most studied pharmacologic treatment, few studies have used a standardized definition of delirium. In addition, few investigations have used reliable and valid delirium symptom rating measures to assess symptom severity before and after intervention. For somatic treatments other than haloperidol, there have been no large, prospective trials or studies including a control group. Information regarding the efficacy of these treatments comes mainly from small case series or case reports; interpretation of the results from many of these case presentations is also made difficult by the use of nonstandardized definitions of delirium or informal measures of delirium symptom severity. Antipsychotics a) Goals and efficacy Antipsychotics have been the medication of choice in the treatment of delirium. Evidence for their efficacy has come from numerous case reports and uncontrolled trials (63, 64). A series of controlled trials also showed that antipsychotic medications can be used to treat agitation and psychotic symptoms in medically ill and geriatric patient populations (6569). However, most of these trials were not conducted with patients who had clearly or consistently defined delirium; in some studies, agitation and disorientation were the sole criteria and symptom assessments ranged from questionnaires to simple identification without symptom descriptions.
Syndromes
Additional information:
Usage: q.i.d.
Tags: topamax 200 mg sale, topamax 200 mg generic, order 100 mg topamax with amex, purchase topamax 200 mg fast delivery
Pavel, 50 years: Having accurate head acceleration data should also help validate various head injury models.
Redge, 64 years: In 1995, Darling and coauthors reported a modified anterior approach to the cervicothoracic junction in a series of four patients with metastatic spinal disease.
Kaelin, 65 years: However, Hodgson and associates reported 40% operative mortality in a series of 10 patients with this technique.