-
(786) 502-2173
-
We've gone mobile!
-
Hours: By Appointment Only
Only $0.32 per item
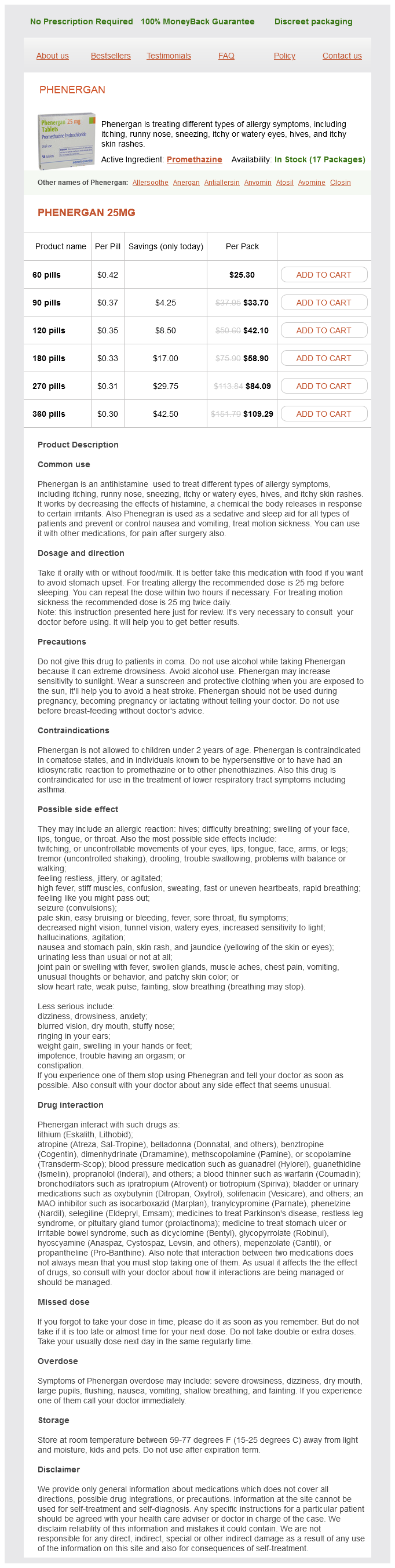
Phenergan dosages: 25 mg
Phenergan packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 831
However anxiety worksheets for teens 25 mg phenergan purchase with visa, consider induced hypothermia (3334°C) treatment in patients who have been successfully resuscitated for cardiac arrest (patients who had ventricular fibrillation or other shockable rhythms). Treatment of severe hyponatremia involves hypertonic saline (3% hypertonic saline, 0. Treatment of hypercalcemia is by saline rehydration infusion, followed by parenteral bisphosphonate pamidronate. The drug, however, is contraindicated in patients with a seizure disorder and in whom concomitant tricyclic antidepressant intoxication is suspected. Hypertonic saline is likely a better osmotic drug, but it requires placement of a central venous catheter first, and valuable time may be lost by placing this catheter first. Mannitol is administered in an initial dose of 12 g/kg (often in two repeated doses, 3045 minutes apart). When performed within 612 hours of onset, the clinical improvement following evacuation of such a mass is often impressive. Initial treatment remains empiric and includes pyrimethamine and sulfadiazine, particularly in patients with multiple abscesses. In endemic areas, patients in coma may have cysticercosis associated with Taenia solium infestation, and immediate treatment with praziquantel is required. It is important to start these treatments early, after consulting an infectious disease specialist. Pressure relief can rarely be accomplished with osmotic agents, and removal of a large bone flap (or flaps) is the only remaining option to salvage the patient with diffuse cerebral edema. An acute hydrocephalus documented by the presence of markedly ballooned ventricles should be treated immediately by placing a ventriculostomy in the right frontal horn. Placement of a ventriculostomy may be precluded in patients on anticoagulation or those with an acquired coagulopathy. Management of Acute Metabolic Derangements and Intoxications As alluded to earlier, with 50 mL of a 50% glucose solution in a suspected hypoglycemic, immediate awakening during infusion is highly indicative of severe hypoglycemia. Failure to awaken after hypoglycemia, however, may indicate that hypoglycemia has been lengthy and has caused significant brain damage, leading to prolonged or no recovery. Management of severe hyponatremia involves hypertonic saline and furosemide (3% hypertonic saline, 0. Overcorrection (> 150 mmol/L) and rapid correction (within 12 hours) have been linked to the development of central pontine myelinolysis. Hypercalcemia is adequately corrected by saline rehydration infusion (34 L), followed by the parenteral bisphosphonate pamidronate (infused at 60 mg over 24 hours). Naloxone has great efficacy but also potentially serious side effects, such as aspiration from rapid arousal and development of a florid withdrawal syndrome characterized by agitation, diaphoresis, hypertension, dysrhythmias, and pulmonary edema. A more prudent approach is to prophylactically intubate the patient and to gradually reverse the overdose of opiates by use of naloxone, 0.
Holly. Phenergan.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96515
The response may vary from minimal asymmetry to pupils failing to constrict or dilate when the penlight moves to the affected eye anxiety symptoms twitching order 25 mg phenergan. In its most pronounced form, pupils dilate immediately when the light shines into the diseased eye. Afferent pupillary defect is linked to optic neuropathy, but a retinal lesion or massive intravitreous hemorrhage (Terson syndrome) may produce similar findings. Optic neuritis is associated with periocular pain and pain with eye movement in 90% of cases. In other patients, optic neuritis may occur after a vaccination or viral illness, or in the setting of connective tissue disease or sarcoidosis. Hereditary optic neuropathy may also present with acute monocular visual loss; and in approximately 50% of patients, family history can be elicited. Certain toxic optic neuropathies have been described; these include methanol, ethambutol, isoniazid, thiamine (B1), and folate deficiency. Diplopia Acute diplopia is complex to analyze, and the underlying deficit may remain ambiguous. Monocular diplopia, almost always due to abnormalities in the refractive media, precludes further neurologic workup. Binocular diplopia is difficult to assess because in some patients multiple cranial nerve involvement is present. Questions that could clarify the chief complaint in acute diplopia should include mode of onset, diplopia disappearing after one eye is closed, whether vertically or horizontally oriented, whether always present or fluctuating, and whether more pronounced in a certain gaze. A survey in the emergency department found, unsurprisingly, that additional neurologic symptoms in a patient presenting with diplopia pointed to a "secondary cause. It is a result of abnormalities in fibers ascending vertically from vestibular nuclei within the medial longitudinal fasciculus. It is important to (a) (b) (c) Nine gaze positions in (a) third-nerve palsy, (b) fourth-nerve palsy, and (c) sixth-nerve palsy (patient follows black dot). Acute oculomotor palsy with preceding retroorbital pain may be a sign of unruptured posterior communicating aneurysm,9 and two-thirds may be smaller than 6 mm; it may herald rupture and indicate rapid aneurysm growth. Funduscopy may demonstrate pulsating venous dilation and, in more extreme forms, disk edema and ophthalmoplegia. Ophthalmoplegia may be due to restricted excursions or cranial nerve injury in the segments traversing the cavernous or petrosal sinus. Visual loss is a consequence of increased intraocular pressure and reversal of flow or thrombus in the superior ophthalmic vein. Complete Ptosis A curious phenomenon is apraxia of eyelid opening (the patient is unable to open the eyes). The abnormality is barely seen but becomes clear with further retraction of the eyelids. Lesions may be at brainstem level, and this condition is more common when brainstem displacement occurs2,6,12 (Chapter 29).
When there are no signs of lead damage and the sensory response is preserved anxiety box phenergan 25 mg with mastercard, parameter settings can be adjusted in attempt to restore efficacy. If all these changes do not lead to any improvement, and all parameters and sensory responses are correct, it is often challenging to find a satisfactory solution. Subsequently, replacement of the lead or contralateral placement of a new lead can be considered. Before definitive placement of a new lead, a test stimulation can be conducted to assess the clinical response. Although this has never been evaluated in clinical studies, data from animal studies suggest a stronger modulatory effect of bilateral stimulation (93, 94). Pain after implantation is not uncommon, occurring in 2434% after long-term followup (1, 5, 30). The physician can attempt to relieve pain symptoms by altering the stimulation settings. Long-term results of a multicenter study on sacral nerve stimulation for treatment of urinary urge incontinence, urgency-frequency, and retention. Efficacy of sacral nerve stimulation for urinary retention: results 18 months after implantation. Stages of vegatative afferentation in reorganization of bladder control during intravesical electrotherapy. The use of electrical devices for the treatment of bladder dysfunction: a review of methods. Studies on the feasibility of urinary bladder evacuation by direct spinal cord stimulation. Neural stimulation for control of voiding dysfunction: a preliminary report in 22 patients with serious neuropathic voiding disorders. Fourth International Consultation on Incontinence Recommendations of the International Scientific Committee: Evaluation and treatment of urinary incontinence, pelvic organ prolapse, and fecal incontinence. Urinary incontinence in both sexes: prevalence rates and impact on quality of life and sexual life. Efficacy of botulinum toxin-A for treating idiopathic detrusor overactivity: results from a single center, randomized, double-blind, placebo controlled trial. Outcome of a randomized, doubleblind, placebo controlled trial of botulinum A toxin for refractory overactive bladder. Predictive factors for sacral neuromodulation in chronic lower urinary tract dysfunction. Patient satisfaction and complications following sacral nerve stimulation for urinary retention, urge incontinence and perineal pain: a multicenter evaluation. Predictors of success with neuromodulation in lower urinary tract dysfunction: results of trial stimulation in 100 patients. Urethral instability and sacral nerve stimulation-a better parameter to predict efficacy
Syndromes
Additional information:
Usage: gtt.
Tags: cheap phenergan 25 mg with visa, purchase phenergan 25 mg amex, phenergan 25 mg buy online, order phenergan 25 mg online
Rune, 46 years: Central representation of bladder and colon revealed by dual transsynaptic tracing in the rat: substrates for pelvic visceral coordination. Several reports about intrinsic pHyp spontaneous activity exist, discharge frequency being detected at values ranging from 13 to 24 Hz (34); in trigeminal autonomic cephalalgias, these recordings revealed tonic, low-frequency, and non-oscillatory patterns of discharge (56). The effect is a result of the proximity of the recurrent laryngeal nerve to the site of stimulation: the recurrent laryngeal nerve initially travels with the main trunk of the vagus before branching at the aortic arch.
Nafalem, 54 years: Injections into the eye What might the benefit be of giving drugs directly into the eye by injection Is the combination of negative computed tomography result and negative lumbar puncture result sufficient to rule out subarachnoid hemorrhage The tonic phase involves flexion of the axial muscles, upward or sideways eye deviation, and marked widening of the pupil diameter with sluggish light responses.
Bram, 51 years: Internet sites are referenced to describe surgery through the use of diagrams and video clips. Apart from a likely benefit effect of valacyclovir or famciclovir (and possibly a corticosteroid course), the treatment is focused on (relatively rapid) escalating doses of opioids, gabapentin, or pregabalin until tolerated. Postural effects Postural effects have been reported relating to changes in stimulation threshold- paraesthesias were felt when in the supine position but were greatly reduced when standing or sitting (13).