-
(786) 502-2173
-
We've gone mobile!
-
Hours: By Appointment Only
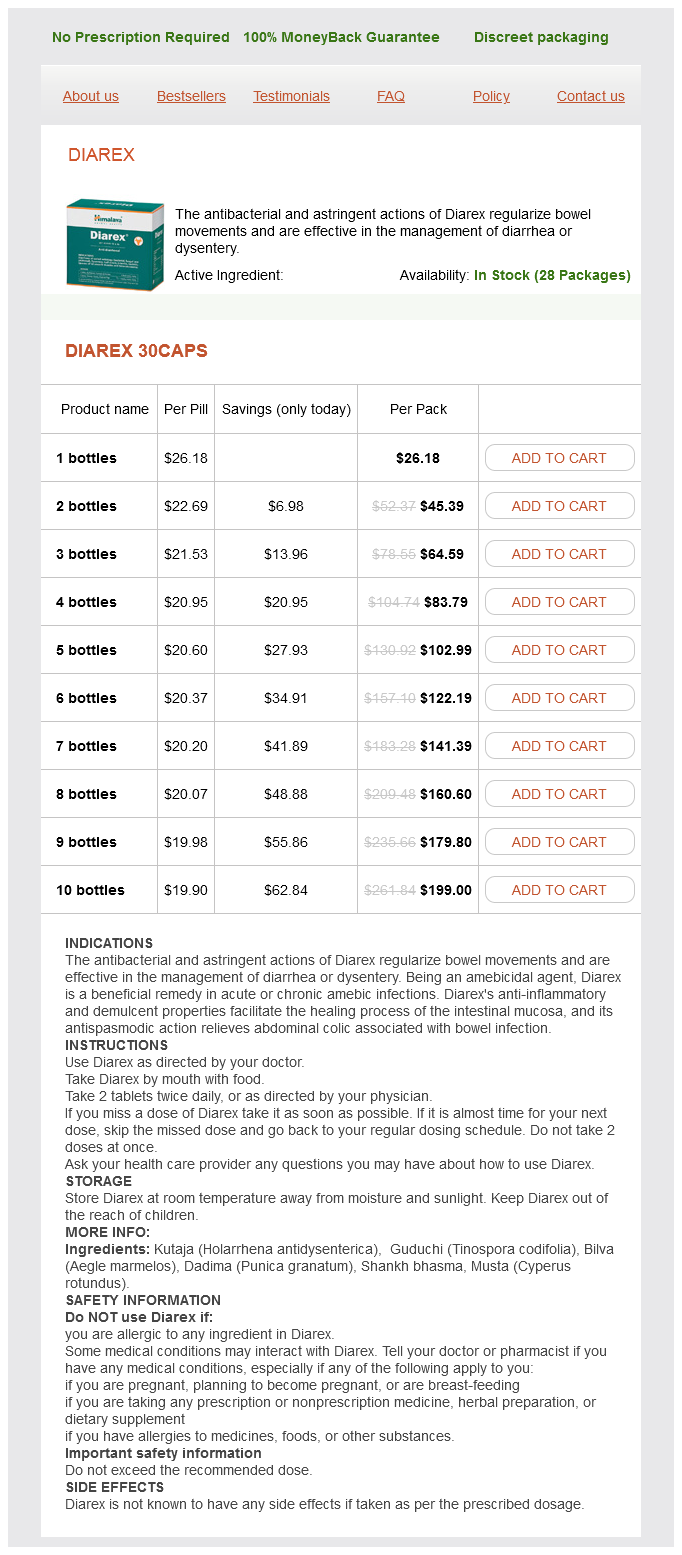
Only $21.14 per item
Diarex dosages: 30 caps
Diarex packs: 1 bottles, 2 bottles, 3 bottles, 4 bottles, 5 bottles, 6 bottles, 7 bottles, 8 bottles, 9 bottles, 10 bottles
In stock: 686
It must be noted that small punctate bleeding that occurs is coagulated using the electrocautery facing away from the plexus gastritis symptoms lump in throat discount diarex 30 caps fast delivery, thereby minimizing the risk of thermal injury to the nerves. Dissection under the coracoid: Visualizing through the D portal and alternating between the I and J portals, the lump of fat under the coracoid is excised using cautery. The cautery is switched from the I to the M portal for complete visualization of the undersurface of the coracoid. These must be meticulously coagulated, as a good view of this region is crucial for completing a coracoid osteotomy. Dissection on the superior surface of the coracoid: the superior surface of the coracoid consists of the remnant of the acromioclavicular ligament and bursal tissue. A global view of the coracoid must be attained while looking in from the I portal. The first assistant controls the arthroscope and a second assistant flexes the arm in neutral rotation, allowing the surgeon to use both hands for completing the steps. The ideal spot should be such that the tip of the guide is roughly 5 mm posterior to the tip of the coracoid. It must be inserted through the skin in oscillation mode to prevent injury to the cephalic vein. The guide wire should be removed prior to advancing the cannulated drill to prevent injury to the plexus. The holes (9 mm apart) are then tapped using the tap provided and the top hats are inserted. Coracoid osteotomy: A 5-mm burr is introduced through the M portal while visualizing through the I portal, and the undersurface of the neck of the coracoid is burred to create a stress riser. A B by inserting the osteotome superiorly and completing the controlled osteotomy. A fresh backflow of bleeding is attained and transient hyperpressure is attained using the pump. Subscapularis split: the arm is adducted and held in neutral rotation without traction, visualizing through the J portal and working through the I portal. This step is mandatory for protecting the axillary nerve and safely completing the subscapularis split. The superior border of the subscapularis is identified adjacent to the rotator interval, and its inferior margin is identified by the anterior circumflex artery and its 2 veins (3 sisters). Creating internal and external rotation, the subscapularis split is made with the electrocautery always pointing away from the axillary nerve.
Luffa cylindrica (Luffa). Diarex.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96230
The radiographic features in this case are typical of congenital pseudoarthrosis of the clavicle-it is almost always on the right side gastritis diet gastritis symptoms 30 caps diarex buy mastercard, in the middle third, with rounded, sclerotic bone ends, and no periosteal reaction. The theory is that vascular pulsations of the adjacent subclavian artery cause failure of the medial and lateral primary centres of ossification to unite. This may explain why congenital pseudoarthrosis of the clavicle occurs on the right in more than 90% of cases (the right subclavian artery is more cephalad as it courses over the first rib), with left pseudoarthrosis occurring more commonly in patients with dextrocardia/situs inversus. Non-accidental injury should always be considered-the odds of clavicle fractures are 4. Other possible differential diagnoses would include cleidocranial dysplasia and neurofibromatosis. It has the highest difference in proximal:distal ratio (the femur is second, with a proximal:distal ratio of 30:70). This, in addition to the thick periosteum of the proximal humerus, the proximity to the physis, and the near universal motion of the shoulder joint, allows fractures in this region to have enormous potential to heal and remodel. Insertion of a medial side K-wire with the elbow in flexion Injury to the ulnar nerve is associated with the fact that in some children with flexion past 90° there is a tendency to sublux the ulnar nerve over the medial epicondyle. Immobilization for 4 weeks in a long arm cast with the elbow flexed to 90° Fractures of the medial epicondyle are common injuries in children and adolescents between the ages of 9 and 14. They account for up to 20% of all elbow fractures in the paediatric population; 60% of cases are associated with elbow dislocation. Management of most medial epicondyle fractures remain non-surgical, generally consisting of immobilization for 4 weeks in a long arm cast with the elbow flexed to 90°. Documented absolute indications for surgical intervention include open fractures and fractured fragments incarcerated in the joint. Relative surgical indications include ulnar nerve dysfunction and valgus instability of the elbow as well as high-demand upper extremity function. Type four fracture of the medial epicondyle: a true indication for surgical intervention. Above-elbow plaster with radiographic review in 57 days to ensure no displacement occurs Fractures of the lateral condyle commonly occur in children aged 510 years. In Milch type I, the fracture extends through the ossification centre of the capitellum and enters the joint lateral to the trochlear groove. In a type I fracture, the articular surface is intact and the fracture is non-displaced and stable. Lateral spur formation Potential complications of lateral condyle fractures include non-union, cubitus varus, osteonecrosis, and protuberance of the lateral condyle. Clinical series report that up to half of cases of lateral condyle fracture have a lateral protuberance. Although there is no functional disability from the protuberance and no surgical treatment is required, it is disconcerting to parents to see the deformity, so it is best to have warned them pre-operatively. The entry point for the ulna should be on the lateral side of the olecranon to avoid ulnar nerve injury. The entry point for the radius is between the first and second compartments (extensor pollicis longus and extensor carpi radialis longus tendons) or between the second and third compartment (extensor carpi radialis brevis and extensor pollicis longus tendons).
At the inferior border of the fundiform part gastritis quick relief generic diarex 30 caps without prescription, the m uscle bers form a V-shaped area called the Laimer triangle. This can result in a Zenker diverticulum, a sac-like protrusion in which food residues m ay collect and gradually expand the sac (with risk of obstructing the esophageal lum en by extrinsic pressure from the diverticulum). In elderly patient s, who can undergo surgeries only to a lim ited extent, the fundiform part of the inferior pharyngeal constrictor m. Note: Because a Zenker diverticulum is located at the junction of the hypopharynx with the esophagus, it is known also as a pharyngoesophageal diverticulum (the term "esophageal diverticulum," while com m on, is incorrect). The anterior part of the pharyngeal wall is interrupted by three openings: · To the nasal cavit y (choanae) · To the oral cavit y (faucial [oropharyngeal] isthm us) · To the laryngeal inlet (aditus) the pharynx is divided accordingly into a naso-, ovo-, and laryngopharynx (see p. B Posterior rhinoscopy the nasopharynx can be visually inspected by posterior rhinoscopy. The angulation of the m irror is continually adjusted to perm it complete inspection of the nasopharynx (see b). The ori ce of the auditory (pharyngot ym panic) tube and pharyngeal tonsil can be identi ed (see p. Orga ns and Their Neurovascula r Structures Tensor veli palatini Levator veli palatini St yloid process St ylohyoid Superior pharyngeal constrictor Salpingopharyngeus Pharyngeal elevators Palatopharyngeus Digastric Masseter Uvular m uscle Medial pterygoid Angle of mandible Middle pharyngeal constrictor Transverse arytenoid Posterior cricoarytaenoid St ylopharyngeus Oblique arytenoid C Pharyngeal musculature Posterior view. This dissection di ers from A in that the m ucosa has been rem oved to dem onstrate the course of the m uscle bers. They form one functional group, which is responsbile for shortening (lifting/elevating) the pharynx when swallowing or closing the epiglot tis. Circular m uscle fibers of esophagus Pharyngeal tonsil Pharyngot ympanic (auditory) tube, cartilaginous part Tubal orifice Tensor veli palatini Medial plate of pterygoid process Pterygoid hamulus Levator veli palatini Salpingopharyngeus Superior pharyngeal constrictor Uvular muscle Palatopharyngeus D Muscles of the soft palate and eustachian tube Posterior view. The sphenoid bone has been sectioned posterior to the choanal opening in the coronal plane, and the following m uscles have been resected on the right side: levator veli palatini, salpingopharyngeus, palatopharyngeus, and superior pharyngeal constrictor. These m uscles are part of the pharynx (space bet ween the soft palate, palatine arches, and lingual dorsum) that form s the posterior boundary of the oral cavit y. The nasal septum, oral cavit y, pharynx, trachea, and esophagus can be identi ed in this dissection. A prom inent part of this defensive ring is the array of tonsils that play an important role in the early recognition of pathogenic m icroorganism s and the initiation of an im m une response (m ore com plex infections spread to the peripharyngeal space, see p. This array consist s of the single pharyngeal tonsil (on the roof of the pharynx), the paired palatine tonsils (bet ween the palatal folds), and the paired lingual tonsils (at the base of the tongue). Additional m asses of lymphatic tissue are located around the pharyngeal ori ce of each pharyngot ympanic (auditory) tube (tubal tonsils) and are continued inferiorly as the "lateral bands. The pharyngeal cavit y is divided into the nasopharynx, oropharynx, and laryngopharynx. The following synonym s for the three pharyngeal levels are in com m on use: Upper level: Middle level: Lower level: Nasal part of pharynx Oral part of pharynx Laryngeal part of pharynx Nasopharynx Oropharynx Laryngopharynx Epipharynx Mesopharynx Hypopharynx 192 Head a nd Neck 5. Orga ns and Their Neurovascula r Structures Soft palate Soft palate Passavant ridge (contracted superior pharyngeal constrictor) Epiglot tic cartilage Thyroid cartilage Cricoid cartilage Oral floor Hyoid bone Thyrohyoid a Epiglot tic cartilage Thyroid cartilage Cricoid cartilage b Oral floor Hyoid bone Thyrohyoid C Anatomy of sw allow ing As part of the airway, the larynx in the adult is located at the inlet to the digestive tract (a).
Syndromes
Additional information:
Usage: gtt.
Tags: diarex 30 caps buy line, 30 caps diarex buy overnight delivery, 30 caps diarex purchase with mastercard, diarex 30 caps purchase without prescription
Ugolf, 35 years: This would prevent subsequent reduction of the posteroinferior glenohumeral ligament to the humeral neck. Articular loss of over 50% is an indication for replacement, especially in the elderly. A meta-analysis examining clinical test utility for assessing superior labral anterior posterior lesions. The optic part of the retina, shown here in yellow, varies in thickness at di erent locations.
Brontobb, 65 years: Plan the arthroscopic procedure and rehearse each suture shuttling step in your mind. As we will see throughout the text, the structures of objects-such as the heart, lungs, or kidneys-determine in large part their functions. Facial nerve Stapedial nerve Geniculate ganglion Trigem inal Hiatus of canal for nerve greater petrosal nerve Trigem inal ganglion Ophthalm ic division Maxillary division Mandibular division Greater petrosal nerve Tym panic cavit y Petrot ym panic fissure Lingual nerve Pterygopalatine ganglion Chorda t ympani St ylom astoid foram en Facial canal Posterior auricular nerve St ylohyoid m uscle Digastric m uscle, posterior belly 1 Internal acoustic m eatus 2 Greater petrosal nerve 3 Stapedial nerve Chorda t ym pani 4 B Branching pattern of the facial nerve: diag nostic signi cance in temporal bone fractures the principal signs and sym ptom s are di erent depending upon the exact site of the lesion in the course of the facial nerve through the petrous bone. It took about ten years for the true nature of the microbe to be understood, and it was given the name "mimi" as an abbreviation for "microbe mimicking.