-
(786) 502-2173
-
We've gone mobile!
-
Hours: By Appointment Only
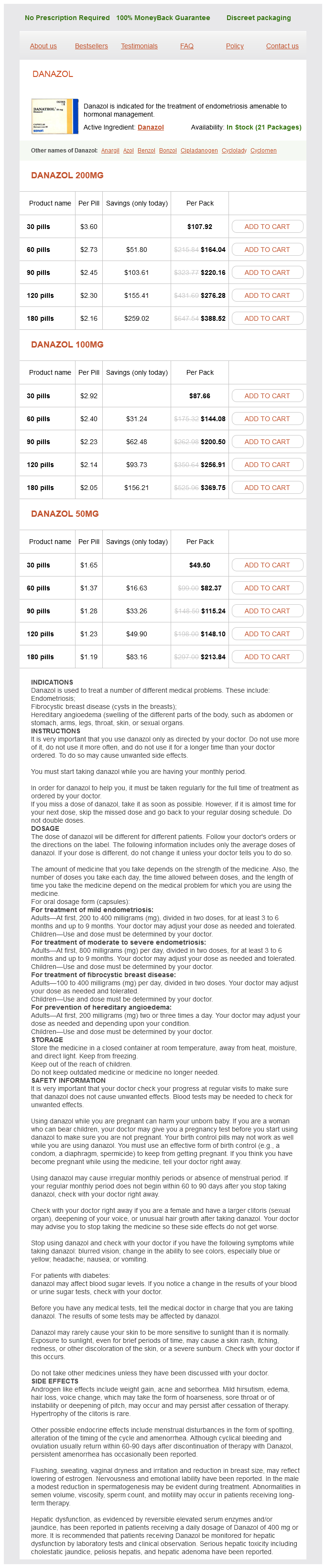
Only $1.26 per item
Danazol dosages: 200 mg, 100 mg, 50 mg
Danazol packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills
In stock: 628
Conversion to a two-stage orchiopexy can be arbitrarily judged by estimating distance of the testicle from the internal inguinal ring and determining a lack of mobility of the spermatic vessels women's health center tualatin discount danazol 50 mg buy line. Dissection of the spermatic cord and testis is done by incising the peritoneum lateral to the spermatic vessels and extending to the internal inguinal ring. The peritoneal dissection leaves a triangle of undisturbed tissue between the vas and the spermatic vessels, preserving collateral vascularity between them. It also has the advantage of allowing a Fowler-Stephens approach if it is found at the end of the dissection that the vessels still have inadequate length. This sign of adequate length is less accurate in older and larger patients, and it is advisable to mobilize more length in an older child. We normally use a 10-mm prescrotal trochar entry for the delivery of the testis into the scrotum. This is done under direct vision from within, along with palpation of the inguinal canal. A laparoscopic grasper is introduced via the scrotum and is used to pull the testis gently to the outside, later to be laid in the subdartos pouch; the skin is then closed with subcuticular stitches. Surgical Technique: Fowler-Stephens Staged Orchiopexy this procedure for high intra-adominal testis can be accomplished very well through laparoscopy. In the first stage, the spermatic vessels are clipped with the help of a 5-mm clip applier at a distance of 5 cm from the testes. Use of a needle to introduce a laser fiber for vessel ablation has also been described. Repeat laparoscopy usually reveals minimal adhesion formation as a result of the initial intervention. Length is usually obtained in a straightforward manner, although excessive traction on the vas deferens should be avoided to prevent damage to the fine vessels and to prevent ureteral obstruction. This technique has demonstrated a good long-term surgical outcome and may be used in patients with bilateral intra-abdominal testes and in those with contralateral testis atrophy after unsuccessful orchidopexy. In most cases, identification of these structures is easy and their removal is straightforward. In some intersex states, the risk for testicular germ-cell tumors is increased more than 100 times, justifying prophylactic gonadectomy as soon as is feasible after the diagnosis is established. If the testes are palpable, orchidectomy can be done through inguinal incisions, but because most of such patients have impalpable testes, laparoscopic exploration and gonadectomy is indicated. In cases of a male pseudohermaphrodite with male gender, resection of müllerian duct derivatives may become necessary.
Butter-Dock (Butterbur). Danazol.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96639
The main difficulty in this surgery is the replacement of the missing urethra (urethroplasty) womens health now discount danazol 50 mg buy online, and various materials have been used without great cosmetic or functional success. The use of scrotal (hairy) skin as free grafts led to serious complications, particularly severe strictures, infections, and urethral stones. Multistage procedures were the fashion for most of the 20th century, with quite unsatisfactory results that resulted in very traumatized patients. In the middle of this dark age of hypospadias surgery, Mathieu, in 1932,29 described a very clever flip-flap procedure to reconstruct distal hypospadias using penile nonhairy skin. It was not until the early 1970s that this surgery changed dramatically, mainly with the work of Asopa,30 Duckett,31 Snyder,32 Ransley,33 and Mollard34 and their colleagues. Well-vascularized urethroplasties using pedicled preputial grafts, preservation of the urethral plate, and the use of free mucosal grafts were important milestones that considerably simplified the surgical approach to hypospadias. Collaboration with endocrinologists, who can stimulate penile growth and healing performances before surgery, also helped greatly in the outcomes of these procedures. Plastic surgeons, who remain involved in hypospadias surgery in some countries, resurrected two-stage procedures using skin grafts in the latter part of the 20th century (Cloutier,39 Bracka40). Correction of Chordee Degloving of the penile skin and freeing of the ventral tissues sitting on each side of the urethral plate usually sorts out the penile chordee related to tethering of the ventral skin and the two spongiosal pillars. If the chordee persists after this first maneuver, freeing of the urethral plate from the ventral surface of the corpora cavernosa, from the glans cap down to the normal urethra surrounded by normal spongiosum, is an alternative advocated by some. In fewer than 5% of cases, the chordee still persists after these two procedures, and a dorsal plication of the corpora cavernosa is then needed. In the most severe form of hypospadias, when a Koyanagi procedure is chosen, the urethral plate is divided behind the glans and detached down to the base of the penis. The plate remains attached distally to the glans cap and is continued proximally by the urethra. Urethroplasty the choice of urethroplasty depends on the quality and width of the urethral plate (the strip of urethral mucosa extending from the ectopic urethral meatus up to the glans cap). The most popular one currently is the Snodgrass procedure, in which the urethral plate is incised longitudinally from the ectopic meatus up to the glans. Alternatively, a rectangle of tissue can be isolated and applied onto the urethral plate and stitched to its edges (onlay urethroplasty). C and D, the rectangle of preputial mucosa is positioned as an onlay on the urethral plate, avoiding circular anastomosis. B, Dissection of the Mathieu flap and incision along each edge of the urethral plate. C, Suture of the Mathieu flap along the edges of the urethral plate over an 8F (2. Penile Covering Once the penis is straight and the urethra has been fully reconstructed, many would advocate covering the neourethra with some healthy tissue, such as the two pillars of spongiosum sitting laterally (spongioplasty) or some cellular tissue taken from the dorsum of the penis or the scrotal region. The next steps are the reconstruction of the new meatus (meatoplasty), the creation of a ventral glans (glanuloplasty), chapter 41: Hypospadias 535 Procedures Using the Urethral Plate Rolling the glanular urethral plate (Thiersch-Duplay procedure)27,28 and covering the reconstructed urethra by means of the two glans wings is a possibility if the glans groove is deep enough.
Given the controversy surrounding the issue of gender assignment women's health clinic amarillo tx 50 mg danazol buy fast delivery, it is not possible at this time to define specific management guidelines. One firm area of consensus is that these decisions must be made in conjunction with parental counseling with full disclosure of all relevant information. If the hindgut remnant is not used for bowel reconstruction, it should be left as a mucous fistula to be used for later bladder augmentation or vaginal reconstruction. Role of Osteotomy Osteotomy is indicated in all children with cloacal exstrophy at the time of bladder closure because of the wide pubic diastasis that is invariably present. Reduction in the incidence of dehiscence and postoperative ventral hernias has been noted in patients treated with osteotomy. In a large series reported by Ben-Chaim and associates,160 significant complications occurred in 89% of patients who underwent closure of cloacal exstrophy without osteotomy, whereas these occurred in only 17% of patients who underwent osteotomy at the time of initial closure. Patients in the two groups were similar in terms of the size of the omphalocele, the presence of myelomeningocele, and the time of primary closure. However, osteotomy had no effect on the eventual continence of cloacal exstrophy patients. Currently, combined anterior innominate and vertical iliac osteotomies are routinely used at our institution. The use of a posterior approach and any complications from this procedure related to the spinal and lower back closure are obviated. In a 1999 series of five patients with extreme pubic diastasis (>10 cm), Silver and coworkers161 described an initial pelvic osteotomy and gradual closure of the pelvic fixator for 1 to 2 weeks, followed by abdominal wall and bladder closure. Closure was successful in all patients without technical problems or surgical complications. This technique of staged pelvic closure also proved reliable in a large series162 for secondary repair of cloacal exstrophy when one-stage pelvic closure was unfeasible. Surgical Reconstruction Complete surgical reconstruction may be considered in an infant who is medically stable. This includes closure of the omphalocele, closure of the bladder and urethra, bony pelvis closure, and repair of the external genitalia. Cloacal exstrophy patients should undergo carefully planned and individualized reconstruction procedures. After closure of the myelocystocele, long-term follow-up is mandatory to evaluate for subtle changes in neurologic examination findings that could herald cord tethering. Once the infant has recovered from closure of the myelocystocele, reconstruction should focus on the management of the gastrointestinal tract. Omphalocele closures are combined with gastrointestinal diversion or reconstruction.
Syndromes
Additional information:
Usage: p.r.n.
Tags: 100 mg danazol order amex, danazol 100 mg fast delivery, danazol 100 mg order amex, order danazol 200 mg visa
Tukash, 27 years: Support groups facilitate two-way transmission of information between patients and physicians that can only be of benefit to both. This supplementary opening should always be catheterized, to exclude a complete duplication.
Emet, 53 years: Theoretically, the routine offer of prenatal diagnosis should decrease postnatal morbidity from renal disease, because early detection allows for rapid initiation of treatment in the postnatal period. Other positive inotropic drugs have consistently reduced survival in chronic failure, and their use is discouraged.
Frithjof, 21 years: During this period, the splenic anlage and the left urogenital fold that contains the gonadal mesoderm are in close proximity. Urinary Defects At birth, the bladder mucosa may appear normal; however, hamartomatous polyps may be present on the bladder surface, representing squamous metaplasia and, commonly, cystitis glandularis.
Musan, 46 years: Confusion arises because the same term is used to describe a pathologic scarring process at the tip of the prepuce in older children and adults, and for some, it always implies pathology. It is interesting that presynaptic inhibitory receptors are present on almost all presynaptic terminals in the brain even though axoaxonic synapses appear to be restricted to the spinal cord.
Faesul, 32 years: Because ureteroceles and some vesical wall abnormalities can be obscured after the bladder is more completely filled, anteroposterior and lateral spot images of the bladder are obtained early during the filling phase. It is also becoming clearer, as we do obtain long-term data, that the results of surgery are often unsatisfactory.