-
(786) 502-2173
-
We've gone mobile!
-
Hours: By Appointment Only
Only $2.04 per item
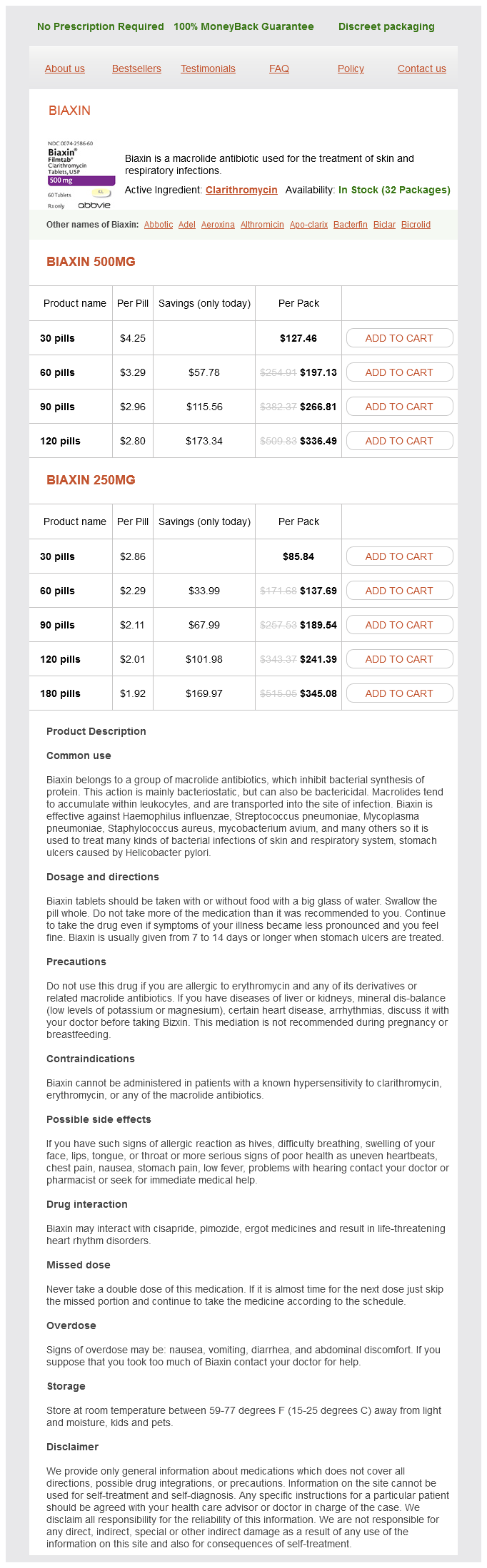
Clarithromycin dosages: 500 mg, 250 mg
Clarithromycin packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills
In stock: 824
The glomerular basement membrane traps most large proteins (>100 kDa) hronicni gastritis symptoms generic clarithromycin 250 mg with mastercard, and the foot processes of epithelial cells (podocytes) cover the urinary side of the glomerular basement membrane and produce a series of narrow channels (slit diaphragms) to allow molecular passage of small solutes and water but not proteins. Some glomerular diseases, such as minimal-change disease, cause fusiown of glomerular epithelial cell foot processes, resulting in predominantly "selective". The fusion of foot processes causes increased pressure across the capillary basement membrane, resulting in areas with larger pore sizes. The combination of increased pressure and larger pores results in significant proteinuria ("nonselective";. Plasma cell dyscrasias (multiple myeloma) can be associated with large amounts of excreted light chains in the urine, which may not be detected by dipstick. The light chains produced from these disorders are filtered by the glomerulus and overwhelm the reabsorptive capacity of the proximal tubule. Renal failure from these disorders occurs through a variety of mechanisms, including tubule obstruction (cast nephropathy) and light chain deposition. Hypoalbuminemia in nephrotic syndrome occurs through excessive urinary losses and increased proximal tubule catabolism of filtered albumin. Common causes of isolated hematuria include stones, neoplasms, tuberculosis, trauma, and prostatitis. Gross hematuria with blood clots is usually not an intrinsic renal process; rather, it suggests a postrenal source in the urinary collecting system. Even patients who are chronically anticoagulated should be investigated as outlined in. Hematuria with pyuria and bacteriuria is typical of infection and should be treated with antibiotics after appropriate cultures. In some of these patients (5060%), reducing calcium and uric acid excretion through dietary interventions can eliminate the microscopic hematuria. The most common etiologies of isolated glomerular hematuria are IgA nephropathy, hereditary nephritis, and thin basement membrane disease. A family history of renal failure is often present in patients with hereditary nephritis, and patients with thin basement membrane disease often have other family members with microscopic hematuria. A renal biopsy is needed for the definitive diagnosis of these disorders, which are discussed in more detail in Chap. Even in the absence of azotemia, these patients should undergo serologic evaluation and renal biopsy as outlined in. Isolated pyuria is unusual since inflammatory reactions in the kidney or collecting system also are associated with hematuria. The presence of bacteria suggests infection, and white blood cell casts with bacteria are indicative of pyelonephritis. In chronic renal diseases, degenerated cellular casts called waxy casts can be seen in the urine. Broad casts are thought to arise in the dilated tubules of enlarged nephrons that have undergone compensatory hypertrophy in response to reduced renal mass. The physiology of water formation and renal water conservation are discussed in Chap.
Red Indian Paint (Bloodroot). Clarithromycin.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96860
Liver function tests should be done prior to the initiation of terbinafine and itraconazole and once a month during treatment gastritis nerviosa buy 500 mg clarithromycin visa. It takes 4 to 6 months for a fingernail and 12 to 18 months for the great toenail to grow out completely. As a result, patients will not see a completely normal nail plate until that length of time has passed. The first sign that treatment is working will be a transition to normal nail plate growth from the proximal nail fold, which, for Laboratory Findings It is important to confirm the diagnosis of fungus prior to initiating treatment. Fungal cultures are not always necessary, but can be helpful in distinguishing between dermatophytes, molds and yeasts. A fungal culture is the least sensitive, but most specific, method for demonstrating a fungal infection. The most sensitive method to detect fungus is to clip the distal portion of the nail plate, place it in formalin, and send it for histopathologic examination. Patients should continue to use antifungal creams on their feet, or powders inside their shoes, at least 3 times a week after treatment with oral medications is completed. In humans, the seborrheic areas (scalp, face, back, and trunk) are always colonized by one or several species of the Malassezia genus. Clinical Presentation History Patients usually present during the summer months with a history of asymptomatic, hypopigmented or hyperpigmented, scaly areas on the trunk. Over the course of time, they may coalesce and cover more extensive areas of the body creating large irregularly shaped patches. Other areas that can be affected include the neck, abdomen, pubis, and intertriginous areas. Hypopigmentation is very conspicuous in dark-skinned individuals and the hypopigmentation may last for weeks or months until the area has repigmented through sunlight exposure. Indications for Consultation · · Patient not responding to treatment Patient preference for physical removal of the diseased nail plates · Underlying nail disease such as psoriasis that requires treatment Patient Information PubMed Health: Cultures are rarely done as it is difficult to grow the fungus on standard fungal culture media. Cutaneous Candida infections generally do not cause significant medical problems, but they can be the source for disseminated candidiasis in immunocompromised patients. Pathophysiology Tinea versicolor is caused by Malassezia furfur and Malassezia globosa, which are saprophytes that normally colonize the skin. In warmer humid weather, the application of these medications may need to be repeated biweekly or monthly to prevent recurrence. Oral antifungals could be used for extensive cases in adults that do not respond to topical treatments. These have a higher incidence of adverse effects and are more expensive18: Ketoconazole 200 mg daily for 7 to 10 days Itraconazole 200 mg daily for 7 days or 100 mg daily for 2 weeks Fluconazole 300 mg as a pulse 1 day a week for 2 to 4 weeks Oral terbinafine and griseofulvin are not effective therapies. Patients should be advised that pigmentation changes will resolve slowly over several weeks with the aid of exposure to sunlight. The patient should be referred to dermatology for severe or persistent disease that does not respond to treatment.
Patients with severe disease may require supportive therapy gastritis diet plan foods cheap 500 mg clarithromycin visa, particularly for pain and dehydration caused by oral mucous membrane involvement. Oral, intravenous, and intramuscular corticosteroids can be used to suppress symptoms. Etiology Drugs Frequency Cause majority of cases Symptoms usually begin less than 1 month and not more than 2 months after culprit drug initiation Examples Antibiotics (sulfonamides, penicillins, quinolones, cephalosporins), anticonvulsants (especially phenobarbital, carbamazepine, lamotrigine), allopurinol (most common cause in Europe and Israel). Features Symptoms Staphylococcal Scalded Skin Syndrome Kids irritable but not too ill; adults often very ill Toxic Epidermal Necrolysis Patients often ill with fever, malaise, and myalgia Skin tenderness varies Severe mucous membrane involvement Blisters with keratinocyte necrosis: often large areas of epidermal erosion Usually drug, occasionally infection Skin tenderness Skin exquisitely tender Mucous membrane involvement Histopathology Clinical correlation Periorificial involvement; mucous membranes spared Blisters in the granular layer with acantholysis; superficial scaling/ desquamation S. Laboratory Findings A skin biopsy is a very helpful tool to confirm the diagnosis and rule out most other mucocutaneous blistering diseases. Later in the disease histopathology shows subepidermal blistering, sparse lymphocytic infiltrate, and full-thickness epidermal necrosis. When submitting a skin specimen for histopathological examination, it is important to do a punch or shave biopsy that includes dermis, submit it in formalin, state the suspected diagnosis, and request for rapid 2- to 4-hour processing. Within in few hours to days flaccid blisters appear and the skin begins to slough, leaving raw denuded areas. Immunobullous diseases such as bullous pemphigoid, pemphigus vulgaris, paraneoplastic pemphigus, pemphigus foliaceus, or linear IgA dermatosis also fall within the differential diagnosis. Patients require a multidisciplinary approach to achieve hemodynamic stabilization, caloric replacement, infection prophylaxis, aggressive skin, eye, and mucous membrane care. Sepsis is the major cause of death and infection surveillance and control are paramount. The most common and severe longterm sequelae are ophthalmologic and include dry eyes, inverted eyelashes, chronic inflammation, fibrosis, and visual loss, including blindness. Physical Examination Pink patches begin abruptly on the face, trunk, and extremities. As they spread they develop flaccid blisters, especially Indications for Consultation Any patient who presents with a severe mucocutaneous blistering disorder should be seen in consultation as quickly as possible. If a dermatologist is not available, the patient should be referred to a facility with a critical care or burn unit for further evaluation. Prompt recognition, elimination of the underlying cause, and aggressive supportive therapy allow the best hope for survival. Damage to the desmosomes causes disruption of cell to cell adhesion in the epidermis and subsequent blistering. The optimal specimen for histopathological examination is a punch or shave biopsy that includes dermis, submitted in formalin for rapid fixation and examination. However, obtaining a skin biopsy in an already uncomfortable child is not always an easy task. Other diagnoses to consider are scarlet fever, Kawasaki disease, and toxic shock syndrome. Erythema with superficial desquamation of skin with crusts and erosions around mouth and eyes.
Syndromes
Additional information:
Usage: q.i.d.
Tags: buy 250 mg clarithromycin overnight delivery, clarithromycin 250 mg purchase with visa, 250 mg clarithromycin purchase with mastercard, discount clarithromycin 250 mg amex
Ali, 45 years: Accentuation in criteria, 3 of 7 organ systems skin folds may be seen, and in must be involved.
Ugo, 27 years: Dehisced wounds can be resutured several days following a closure if the wound is cleaned and any risk for infection is addressed.
Sinikar, 40 years: Stage Ib: the invasion of the malignant cells to the underlying stroma exceeds 5 mm.
Sven, 63 years: Gram-negative folliculitis presents with pustules on the central face and may closely resemble acne.
Stejnar, 36 years: Growth factors or granulocyte colony-stimulating factor are used to prevent hemorrhagic toxicity of chemotherapy.
Kippler, 30 years: Radiation therapy is used for large macroadenomas and for cases with large residual tumor after surgery.
Uruk, 59 years: Calcineurin inhibitors in pediatric atopic dermatitis: a review of current evidence.