-
(786) 502-2173
-
We've gone mobile!
-
Hours: By Appointment Only
Only $1.52 per item
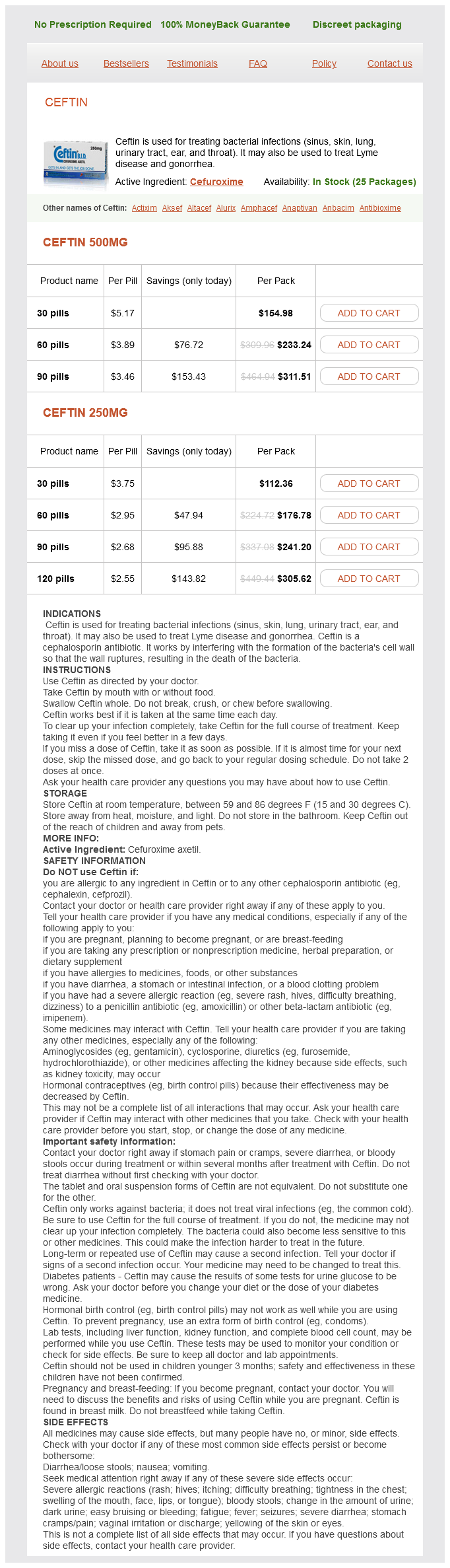
Cefuroxime dosages: 500 mg, 250 mg
Cefuroxime packs: 30 pills, 60 pills, 90 pills, 120 pills
In stock: 833
These two types of fibers may be inhibited by stimulation of the adjacent thickly myelinated and fast conducting (A) fibers treatment 30th october cefuroxime 250 mg buy without a prescription. In contrast, the thinly myelinated and unmyelinated fibers are excitatory to the T cells and inhibitory to the interneurons of the substantia gelatinosa, which, in turn, presynaptically inhibit the afferents that synapse with the T cells. Stimulation of the thinly myelinated or unmyelinated afferent fibers inhibits the interneurons of the substantia gelatinosa, preventing them from inhibiting the T cells and thus opening the gate for nociceptive impulses that ascend to the ventrolateral thalamic nucleus. Inhibition of transmission is aided by supraspinal descending inhibitory pathways. Neuronal sensitization is associated with transmission of noxious stimuli that seems to occur at the peripheral terminals and at the central synaptic sites in the dorsal horn of the spinal cord. At the peripheral or receptor endings, increased sensitivity does not only occur at the traditional nociceptor endings but also at those mechanoreceptors and thermoceptors that are activated subsequent to inflammatory process. At the synaptic sites in the dorsal horn, processing of the nociceptive information is accomplished by lowering the threshold of spinal neurons that receive the afferent through prolonged repetitive facilitatory effect of incoming afferent fibers after a brief stimulation. The above facts about central sensitization and neuronal plasticity may enable the development of medications that address the issue of hyperalgesia at the spinal level and hyperexcitable neurons and thus maintain normal signaling pattern. The nucleus raphe magnus in the medulla, the neurons of the medial reticular zone, and the periaqueductal gray matter constitute a system that provides endogenous analgesia. Note the ipsilateral course of this pathway in the spinal cord and contralateral course at supraspinal levels. Transmission of pain occurs as a result of imbalance between the afferent impulses that reach the spinal gray matter in the presence of massive afferents through the thinly myelinated fibers. This is a contralateral pathway that shows reverse somatotopic arrangement to that of the dorsal column. Other pathways associated with transmission of pain such as spinoreticular are also illustrated. These neurons receive input from the cerebellum, the periaqueductal gray matter, and the spinal cord, conveying efferent fibers to the spinal trigeminal nucleus at the brainstem level and to the substantia gelatinosa at the spinal level to modulate nociception. Similarly, efferent fibers from the periaqueductal gray matter project to the spinal neurons as well as the ponds and medulla. Nociceptive impulses for the most part are carried by the A and C fibers that ascend one or two segments above the level of their entry in the dorsolateral tract of Lissauer and then synapse in certain Rexed laminae of the spinal cord; others, although few, may establish synaptic connections at the same level of their entry into the spinal cord. However, not all nociceptive fibers contribute to the lateral spinothalamic tract; in fact, some may synapse on interneurons that send processes to inhibit the C and A fibers by secreting enkephalins. The dorsal portion of this tract transmits temperature, whereas the ventral portion conveys pain sensation. Visceral pain fibers occupy the most medial part of the lateral spinothalamic tract, adjacent to the gray matter.
Edible date (Date Palm). Cefuroxime.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96434
The origin and distribution of this pathway is somatotopically organized with fibers emanating from the rostroventral medications adhd discount cefuroxime 250 mg line, central and dorsocaudal parts of the lateral vestibular nucleus projecting to the cervical, thoracic and the lumbosacral segments, respectively. It is monosynaptically and polysynaptically excitatory to the alpha motor neurons of the extensor muscles in the extremities, trunk, and neck. The ascending component includes the vestibulo-ocular fibers, which project bilaterally to the motor nuclei of the oculomotor, trochlear, and abducens nerves as well as the axons of the internuclear neurons of the contralateral abducens nucleus. These fibers mediate the vestibulo-ocular reflex, coordinate the contraction of the extraocular muscles, and fixate our gaze during head rotation. In the vestibulo-ocular reflex, impulses generated from the vestibular nuclei and mainly the medial vestibular nucleus. The activated (right) abducens nucleus sends commands via the internuclear neurons to the neurons of the medial rectus muscle of the contralateral (left) oculomotor nuclear complex that produces adduction of the left eye and to the ipsilateral motor neurons of the (right) abducens nucleus that causes abduction of the right eye. Activation of the abducens internuclear and abducens motor neurons produces movement of both eyes to the side of the original stimulus. As mentioned earlier, abducens internuclear neurons mediate conjugate adduction of one eye with the abduction of the opposite eye in lateral gaze. The vertical gaze center is also activated by the input generated from the medial vestibular nucleus. This occurs when bilateral movement of the endolymph into the superior ampullae (during neck flexion) and inferior ampullae (during neck extension) activate the corresponding ampullae, and subsequently, the medial vestibular nuclei. To view an object of interest, both eyes have to be directed conjugately toward the target. Activation of the internuclear and multipolar neurons within the abducens nucleus produces deviation of the eyes toward the right side or the side of the stimulated abducens nucleus. A lesion of the frontal eye field disrupts the neural circuit that mediates conjugate deviation of the eyes toward the opposite side. As a result the contralateral frontal eye field will be dominant, and both eyes conjugately deviate toward the side of the lesion. If the cortical lesion is extensive enough to also involve the precentral gyrus and the ensuing corticospinal tract, the patient exhibit manifestations of contralateral upper motor neuron palsy and conjugate deviation of both eyes toward the same side, as seen in comatose patients. Note that the vestibular input to the abducens nucleus through lateral gaze center and ensuing impulses act upon the medial and lateral rectus muscles through the associated neurons. In summary: vestibular receptors peripheral processes of the vestibular neurons vestibular ganglia primary vestibular fibers vestibular nuclei cerebellum. The postsynaptic fibers from the vestibular nuclei also form the secondary vestibular fibers that project to the spinal cord, motor nuclei, and cerebellum. Below are some of the most important conditions associated with vestibular dysfunctions. A unilateral lesion that disrupts the vestibular nerve produces an imbalance of the vestibular input, causing overstimulation of the contralateral vestibular nuclei accompanied by an equal increase in the discharge of the contralateral vestibular nerve.
Some patients developed dystonia and athetoid movements as complications of neurosurgical intervention treatment uti infection discount cefuroxime 500 mg buy on-line. Posteroventral pallidotomy reemerged as a method of treatment developed by Leksell, which achieved good relief from tremor, rigidity, and akinesia. However, central homonymous visual field deficit, facial weakness, and dysphasia are the Extrapyramidal Motor System 475 reported complications of this procedure. In view of the fact that the brain is an immunological privileged site, attempts to experimentally transplant mesencephalic fetal cells were carried out, though with no clear-cut success. Chorea is a brisk, rapid, graceful, and purposeless movement of short duration, unpredictable in direction, timing, and location, which starts suddenly and shows no rhythm. These movements are parakinetic, which appear to be meaningful, but in reality, they do not serve any rational purpose. They may occur in isolation or may be accompanied with other involuntary movements. Chorea may be confined to one side of the body (hemichorea) or specific muscles, for example, respiratory muscles (respiratory chorea). Diffuse degenerative process in the neostriatum may result in choreiform movement intermixed with tics, parkinsonism, and dystonia. These movements show exacerbation under stressful situations and during walking, persist as long as the patient is awake, and may even continue during sleep. Twitching in the face, lip-smacking or pouting, cheek puffing, tongue rolling, and jaw protrusion usually accompany the involuntary movements. Patients may not be aware of these involuntary movements and may be thought of as fidgeting or being clumsy. Hypotonia, a decrease in the muscle tone or atonia, which occurs at the end of each involuntary movement, may lead to a delay in the relaxation of the contracted muscles. Ocular disorders (disruption of saccades and gaze abnormalities) and jerky finger-to-nose testing also occur. Chorea is considered as a manifestation of impairment of the modulatory effect of the basal nuclei upon thalamocortical projections and receptor blockade of the neurotransmitter. The putamen, the globus pallidus, and the subthalamic nucleus play an important role in the development of chorea. In healthy individuals, efferents from the subthalamic nucleus utilize a glutamate excitatory pathway in its excitatory projection to the globus pallidus and the substantia nigra. This pathway excites the pallidal neurons that project to the thalamus and thus inhibits corticothalamic projection to the motor cortex. In patients with chorea, the excitatory subthalamic projection is reduced or abolished, producing disinhibition of the pallido thalamic projection. The pathogenesis of this disease is based on the fact that streptococcal M proteins induce the production of antibodies (IgG) against neurons of the caudate nucleus and subthalamic nucleus, disrupting their function. It should be differentiated from dystonia, tic disorders, and dyskinesia associated with drug withdrawal. The involuntary movements are uncoordinated, are more rapid than those of Huntington chorea, and may have a lightning character.
Syndromes
Additional information:
Usage: b.i.d.
Tags: 250 mg cefuroxime, cefuroxime 250 mg buy on line, cefuroxime 250 mg generic, 500 mg cefuroxime order
Joey, 27 years: Also, monitor fluid intake and output; decreasing urine output may indicate nephrotoxicity. The precommissural part corresponds to the paraterminal gyrus lodged between the posterior paraolfactory sulcus and the lamina terminalis, continuing with the diagonal band of Broca, medial olfactory stria, and induseum griseum.
Mezir, 33 years: Antigen localization in a tissue depends on several factors, most notably the cellular disposition of the antigen. Functional loops and pathways It has been suggested that several loops, with closed and open components, are involved in the connections of the basal nuclei.