-
(786) 502-2173
-
We've gone mobile!
-
Hours: By Appointment Only
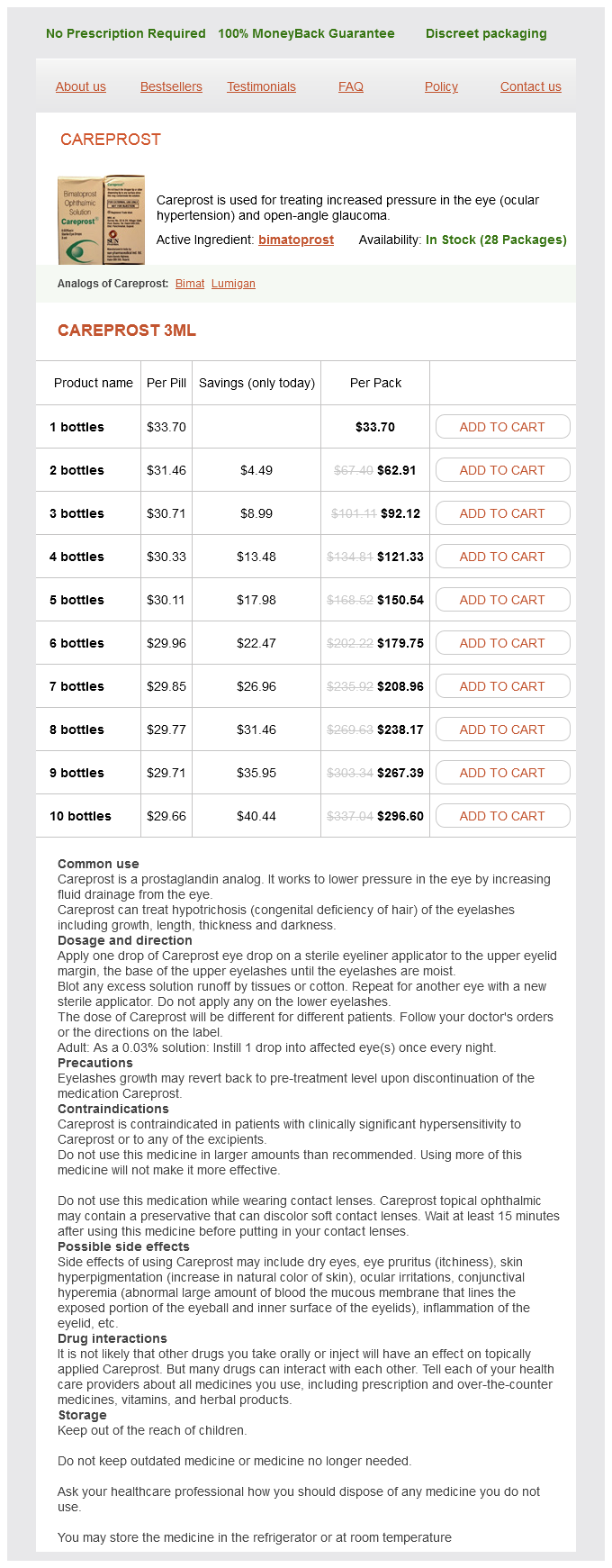
Only $31.51 per item
Careprost dosages: 3 ml
Careprost packs: 1 bottles, 2 bottles, 3 bottles, 4 bottles, 5 bottles, 6 bottles, 7 bottles, 8 bottles, 9 bottles, 10 bottles
In stock: 910
Lip cancer is usually detected in its early stages due to its conspicuous anatomic location brazilian keratin treatment 3 ml careprost visa. Cancers arising from the dry vermilion that arise from areas involved by actinic cheilitis tend to be slow growing. Surface changes that are thought to be due to actinic cheilitis may in fact be involved by early invasive cancer that remains undiagnosed until vermilionectomy is performed. Subtle actinic-appearing changes, if untreated, may slowly progress to a raised irregular exophytic lesion, an indurated subcutaneous/submucosal lesion, or an ulcerated lesion. The involved mucosa may have a patchy appearance with areas of normal-appearing mucosa. Biopsy of a necrotic central ulceration may result in a false-negative biopsy result, so biopsy of viable tissue surrounding the central ulceration is preferred. Clinical evaluation requires careful inspection of the surface anatomy of the lip to characterize any changes of the dry and wet vermilion. Examination for mottling, color and textural changes, fissuring, ulcerations, induration, and obscuration of the vermilion border and normal lip anatomy should be performed. Incisional or punch biopsy is preferred over shave biopsy, which could lead to the incorrect diagnosis of a noninvasive in situ lesion. Physical examination of the lip and neck is sufficient for smaller lesions, whereas axial imaging should be considered for lesions measuring more than 2 cm in diameter. Information pertaining to retrograde perineural involvement of the trigeminal nerve and mandibular marrow invasion is ideally assessed with magnetic resonance imaging. While the updated staging criteria reflect our current understanding of lip cancer, they will also result in stage migration that limits our ability to extrapolate treatment outcomes from the existing peer-reviewed literature to the updated stage groups. Most retrospective case series document metastasis rates of less than 15% in lesions measuring 4 cm or less. Zitsch et al documented cervical metastasis in 7% of patients 2 cm or less in diameter versus 16% in larger cancers. A large retrospective review of 1,036 lip cancers found that 31% of cancers involving the commissure metastasized to the cervical 13. Wider tumor-free margins are essential to maximize local control and to minimize the need for adjuvant radiotherapy with or without chemotherapy. Individuals who wear removable dentures must be counseled that postoperative microstomia may prevent their use. Careful preoperative assessment with inspection and palpation permits the surgeon to appreciate the three-dimensional nature of the cancer, the planned resection, and the resultant soft-tissue defect. Lip cancer resection should be performed en bloc with the intent to achieve negative, or clear, margins during the initial resection. The excision of lip cancers with 10-mm mucosal margins that are immersed in 10% buffered formalin shrink by 41 to 47. Resection of the lip cancer and vermilionectomy of the entire lower lip was performed.
Glutamine. Careprost.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96846
The amount and degree of residue in the valleculae and pyriform sinuses are assessed in lateral and frontal planes treatment 1860 neurological proven 3 ml careprost. Finally, one can visualize cricopharyngeal relaxation and assess for the ability of the bolus to pass to the esophageal phase. It is also important to inquire whether these patients have lasting sequelae including dysphagia, xerostomia, dysgeusia, lymphedema, trismus, and fibrosis. Prior oral surgical resections should also be considered as there may be a degree of baseline altered anatomy and speech and/or swallowing dysfunction. When there are unilateral deficits, optimal placement of foods and liquids on the unaffected side can be extremely helpful. All of these considerations would be indications to perform instrumental swallowing evaluations preoperatively, rather than just a clinical swallowing and oral motor evaluation. Therapy is not necessarily indicated, given that speech and swallow functions are likely to change postoperatively. However, postoperative treatment planning and goals are discussed in the preoperative evaluation. The anticipated need for swallowing, speech, and/or trismus therapy is reviewed with the patient. This has shown to be beneficial in improving postoperative patient compliance and understanding of their postoperative needs. While the exact outcomes are often difficult to predict, patients are often reassured that with time and therapy, the goal is to establish the best possible speech and swallowing given the amount and nature of resection, reconstruction, and affected structures. To improve patient understanding and reassure them that the goal is best possible functional outcomes. Oral cavity and oropharyngeal cancer incidence trends and disparities in the United States: 20002010. Factors affecting swallow outcome following treatment for advanced oral and oropharyngeal malignancies. Counseling issues: addressing behavioral and emotional considerations in the treatment of communication disorders. Functional and quality of life outcomes after partial glossectomy: a multi-institutional longitudinal study of the head and neck research network. Effect of preoperative counseling on hospital length of stay and readmissions after total laryngectomy. Cancer prehabilitation and its role in improving health outcomes and reducing health care costs. Tumor size and pretreatment speech and swallowing in patients with resectable tumors. Tumour boards/multidisciplinary head and neck cancer meetings: are they of value to patients, treating staff or a political additional drain on healthcare resources Multidisciplinary head and neck cancer clinic and adherence with speech pathology. The primary benefit of a flap in the case of oral tongue resections is both cosmetic and functional.
If no fluid is obtained symptoms kidney failure 3 ml careprost buy with amex, if the cyst re-forms within 2 weeks or must be repeatedly aspirated, or if a mass persists after the aspiration, biopsy should be performed. Asymptomatic cysts in women younger than 40 years do not require treatment; in patients older than 40 years, biopsy is indicated. Mild Bartholin gland infections may also be treated with broad-spectrum antibiotics and frequent warm sitz baths. When an acute abscess is to be drained, the exquisite tenderness that is usually present dictates that this is gently performed; pain relief is best obtained by using an analgesic or skin-freezing spray. This technique may also be used for nonacute Bartholin cysts; local anesthesia using local or field infiltration is also appropriate. Abscesses should be incised at the point of least thickness overlying the mass (where the abscess is "pointing"). A vertical or "stab" incision is made, generally resulting in the abrupt release of purulent material. The size of this incision need only be of the order of 1 or 2 cm; sutures are generally not required. The abscess cavity may be gently irrigated with normal saline using a 10-mL syringe. A Word catheter should then be placed through the incision and inflated with a few milliliters of saline. When the cyst is not acutely inflamed, it should be stabilized and tensed by gentle finger pressure applied on either side of the affected labium, below the cyst. Incision length should be similar to that used for acute cases, and a Word catheter or iodoform gauze packing should be inserted in a similar manner. Iodoform gauze packing should be gradually removed over the course of several days. Recurrence is frequent, and many prefer marsupialization to simple drainage in all but the most acute cases. Prospective randomized study of marsupialization versus silver nitrate application in the management of bartholin gland cysts and abscesses. Core needle biopsy may not be suitable for patients who have very small or very hard breast lumps; masses close to the chest wall, nipple, or surface of the breast; calcifications that require magnification; or very small breasts. Patients who take blood thinners or aspirin should discontinue them before the procedure. Women who cannot remain still or in the supine position for 2040 minutes because of physical illness or other problems are not good candidates for stereotactic core needle biopsy. The patient may be either in the supine or prone position based on the location of the lesion to be biopsied, optimal access, and availability or need for image guidance. Using the fingers of the opposite hand to stabilize the area in question, the physician advances the needle into the area of concern by palpation or under image guidance using either stereotactic mammography or ultrasonography. Passage of the needle through the skin may be facilitated by a small incision if desired.
Syndromes
Additional information:
Usage: q.3h.
Tags: purchase 3 ml careprost otc, purchase careprost 3 ml mastercard, careprost 3 ml buy visa, 3 ml careprost free shipping
Thorek, 65 years: Specific complications-early · Per-operative ureteric or rectal injury (both rare, <0.
Milten, 61 years: Interpretation · results can be roughly graded as: · 0, no response; · 1+, erythema and oedema; · 2+, erythema, papules, and small vesicles; · 3+, marked erythema, induration, and large blisters.
Ronar, 52 years: The incidence of early primary site disease varies widely, with the incidence of patients presenting with primary tumors 4 cm ranging from 18 to 91% in the literature.
Marcus, 46 years: When possible, we often displace uninvolved oral cavity structures away from the anticipated radiation field to minimize treatment-related toxicity.
Umul, 24 years: Small T1 lesions can be resected and closed primarily with local tissue rearrangement or a small skin graft.
Gonzales, 59 years: On one hand, Mücke et al showed adding neoadjuvant chemotherapy to osteosarcomas improves survival.