-
(786) 502-2173
-
We've gone mobile!
-
Hours: By Appointment Only
Only $0.18 per item
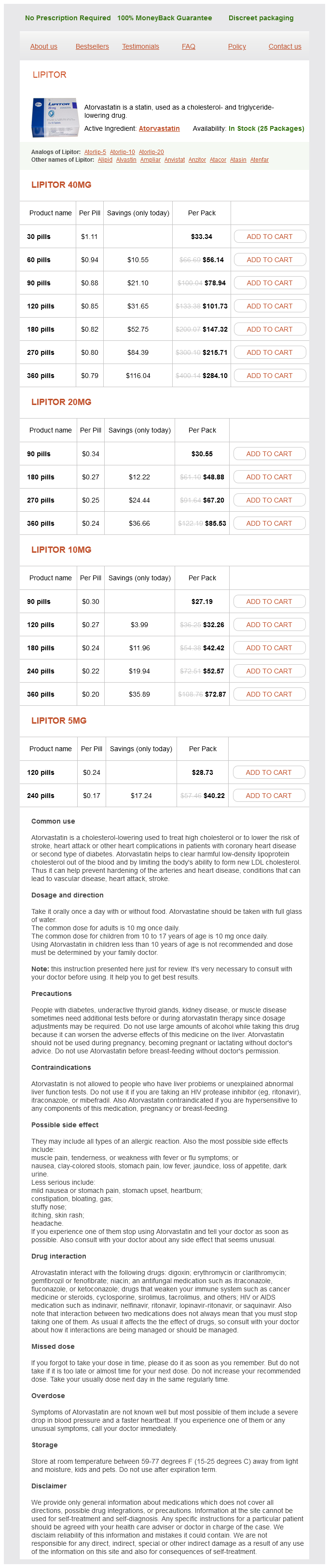
Atorvastatin dosages: 40 mg, 20 mg, 10 mg, 5 mg
Atorvastatin packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills, 240 pills
In stock: 557
Hypertension after pediatric cardiac transplantation: detection cholesterol table 40 mg atorvastatin purchase with mastercard, etiology, implications and management. Determinants of renal function in pediatric heart transplant tecipients: long-term follow-up study. Pulmonary Vascular Disease Pathophysiology of Pulmonary Hypertension Marlene Rabinovitch T his chapter addresses the pathophysiologic mechanisms leading to pulmonary hypertension associated with congenital heart defects and other disease-related or idiopathic processes. A variety of physiologic factors appeared to contribute to the severity and rate at which vascular disease developed in patients with congenital heart defects (Table 66. Patients with cyanotic heart defects who had large, surgically created systemic-to-pulmonary artery shunts were also at risk for pulmonary vascular disease. Several investigators tried to quantify the degree of medial hypertrophy, but their measurements did not correlate closely with the preoperative level of pulmonary vascular resistance or with its change postopera ti vel y (3). Structural Remodeling and Growth Beginning in 1965, a new and quantitative method of analysis of the pulmonary vascular bed was developed that was particularly applicable to the study of infants and young children because it incorporated features of altered growth of the pulmonary circulation. This method was based upon extensive studies carried out using a technique of radiopaque barium-gelatin arterial injection of a postmortem lung specimen. It was observed from the postmortem arteriograms that the vessels are prominent in the newborn, whereas in the adult they are obscured by a dense background haze produced by the addition of many small intra acinar arteries not present at birth (4). On microscopic examination, three features of normal remodeling and growth of the pulmonary vascular bed were established (5). At birth, the muscularized arteries are thick walled, but within a few days, the smallest muscular arteries dilate and their walls thin to adult levels. Although alveoli also proliferate, the ratio of alveoli to arteries actually decreases from the newborn value of 20:1 to the value of 8:1, which is achieved first in early childhood and which persists. Morphometric analysis of the lungs of patients with congenital heart defects reveals disturbed growth and remodeling of the pulmonary vascular bed (Table 66. On microscopic examination of the pulmonary vascular bed, muscle had extended precociously into normally nonmuscular peripheral arteries, regression of the perinatal musculature had not occurred, and there was additional medial hypertrophy. Because there were no regional variations in the lung, it was feasible to apply the morphometric technique to analysis of lung biopsy tissue in assessing abnormal muscularity and evaluating arterial size and number (7). Medium is thickened as a result of fasciculi of longitudinal muscle, and vessel is all but occluded by fibroelastic tissue. There is cellular intimal proliferation (arrow); clustered around are numerous thin-walled vessels that terminate as capillaries in the alveolar wall. With grade B, as in grade A, there is increased extension of muscle, but, in addition, there is more severe medial hypertrophy of normally muscular arteries. We correlated the quantitanve features of abnormal growth and remodeling of the pulmonary arteries and the qualitative changes described by Heath and Edwards with the hemodynamic behavior of the pulmonary circulation in the immediate postoperative period In the intensrve care unit 1 day after repair and at the time of routine cardiac catheterization study 1 year later (9).
Pyruvic Acid (Pyruvate). Atorvastatin.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96084
Some have no skeletal muscle dystrophin abnormality but have abnormalities of the cardiac dystrophin (14 cholesterol juice recipes order 10 mg atorvastatin with amex,91-93). Other studies have shown a mild decrease in skeletal muscle dystrophin with normal distribution, but no dystrophin was found in heart muscle (94). Of note, female carriers can show heart failure that is slowly progressive and often fatal (95). The progressive fibrous and fatty depositions mainly involve the atria, ultimately causing mechanical and electrical atrial paralysis. Some patients will have late ventricular dilation, severe congestive failure, and arrhythmias. Pacemaker implantation can be lifesaving, but late deaths have happened even in patients who have pacemakers (7,105-115). Patients may complain of sleep disturbances and gastrointestinal problems, both constipation and diarrhea, before developing muscle weakness. Progressive facial muscle, temporalis, sternocleidomastoid, and limb weaknesses develop along with cataracts (77). The weakness is unique among the common muscular dystrophies, affecting distal equal to or greater than proximal muscles. Patients also can have frontal baldness, diabetes, and frequently, infertility (97). When Steinert (98) described the disease, he noted that patients often had a slow pulse rate. Cardiac ventricular diastolic and systolic duration in children with heart failure secondary to idiopathic dilated cardiomyopathy. Survival in Duchenne muscular dystrophy: improvements in life expectancy since 1967 and the impact of home nocturnal ventilation. Observations of the cardiovascular involvement, including the cardiac conduction system, in progressive muscular dystrophy. The incidents of severe anesthetic complications in patients and families with progressive muscular dystrophy of the Duchenne and Becker types [in German]. Electrocardiographic abnormalities and arrhythmias are strongly associated with the development of cardiomyopathy in muscular dystrophy. Echocardiographic and electrocardiographic findings of cardiomyopathy in Duchenne and Becker-Kiener muscular dystrophies. Genetic predictors and remodeling of dilated cardiomyopathy in muscular dystrophy. Sequential changes in cardiac structure and function in patients with Duchenne type muscular dystrophy: a twodimensional echocardiographic study. The relationship between clinical stage, prognosis and myocardial damage in patients with Duchenne-type muscular dystrophy: five-year follow-up study. Prevalence and distribution of regional scar in dysfunctional myocardial segments in Duchenne muscular dystrophy.
The finding of a subsystemic right ventricular pressure is consistent with a globally disadvantaged right ventricle canadian cholesterol ratio guidelines generic atorvastatin 20 mg visa. The right ventricle is usually thinned, and severe tricuspid regurgitation often is present. The functional disturbance of severe tricuspid regurgitation correlates with an Ebstein-like abnormality of the tricuspid valve or severe tricuspid valve dysplasia. When right ventricular angiography does not demonstrate ventriculocoronary connections, one can be reasonably certain that coronary arterial stenosis or interruption or major fistulae with coronary-cameral flow will not be evident. In some patients with ventriculocoronary connections, a balloon catheter inflated in the right ventricle or catheter-induced tricuspid insufficiency with concurrent observation of the simultaneous electrocardiographic tracing may unmask a right ventricular-dependent coronary circulation. The angiocardiographic investigation of the patient with the hypertensive right ventricle requires right ventricular angiocardiography in frontal and lateral projections. The reported surgical survival of 27% prior to the availability of prostaglandins was poor (57). Rarely an urgent balloon atrial septostomy may be required for a restrictive septum as pulmonary flow improves and should be considered in any neonate that demonstrates persistent low cardiac output with the usual therapeutic maneuvers. For the premature infant or the extremely small-for-gestational-age infant, a prolonged course of an E-type prostaglandin may be necessary before surgery is undertaken, although this is unusual in the current surgical era. Once pulmonary blood flow is established, it is important to recognize that systemic oxygen saturation is related to the amount of flow into the pulmonary circulation. The patient has an obligatory rightto-left shunt at atrial level, hence a very high saturation usually reflects an enormous amount of pulmonary flow. The resulting low diastolic pressure and low cardiac output syndrome can result in compromised splanchnic and renal flow as well as ongoing acidosis and, in the extreme, cardiogenic shock. In addition, this physiology can compromise oxygen delivery to the aortocoronary circulation resulting in myocardial ischemia. The pulmonary outflow tract in this patient with valvar atresia is imaged in the precordial short-axis view with slight clockwise rotation. Lower Panel: the possibility of pulmonary insufficiency (red flow) raises the possibility that the valve is severely stenotic and not atretic. Selective injection of the right ventricular outflow tract can differentiate severe stenosis of the pulmonary valve from membranous atresia (56). Aortography in the neonate defines the laterality of the aortic arch, the caliber of the subclavian arteries, the site of insertion of the arterial duct, the caliber of the pulmonary arteries, and coarctation of the pulmonary artery at the insertion of the arterial duct that may preclude treatment with a stent to permanently maintain its patency or require a surgical patch at the time of placing a Surgical Surgical and other catheter-based interventional therapies have continued to change with an understanding of the heterogeneity of this disorder. The diagnostic and therapeutic algorithms are now quite diverse, depending on a wide number of morphologic variables (5,58-62). Among some centers, primary cardiac transplantation also is considered particularly when the coronary artery anatomy is complex.
Syndromes
Additional information:
Usage: q.3h.
Tags: discount atorvastatin 10 mg on line, discount atorvastatin 20 mg buy, buy cheap atorvastatin 20 mg line, 5 mg atorvastatin buy
Thorek, 31 years: It is noteworthy that in some parts of the world, monoarticular arthritis is a common mode of presentation (136,153). Tricuspid valve abnormalities are common and can include a bileaflet valve, tricuspid valve dysplasia/prolapse, and abnormal papillary muscle arrangements (81). Head size at birrh in neonates with transposition of great arreries and hypoplastic left hearr syndrome. The degree of ascending aortic and arch hypoplasia is less than that observed with aortic atresia.
Hassan, 25 years: Evaluation of Quality of Life in Children and Adolescents with Congenital and Acquired Heart Disease Bradley S. Diagram of congenitally corrected transposition of the great arteries demonstrating atrioventricular and ventriculoarterial discordance. These newer understandings about the diseases and their nuances will ultimately lead to improved diagnosis and likely different classifications and therapeutic approaches. One death was caused by aortic rupture, and one was related to a cerebrovascular accident.
Ivan, 27 years: From the suprasternal long-axis view, typical thoracic coarctation appears as a localized narrowing of the thoracic aorta just beyond the origin of the left subclavian artery. Tricuspid valve abnormalities are common and can include a bileaflet valve, tricuspid valve dysplasia/prolapse, and abnormal papillary muscle arrangements (81). New understanding about calcific aortic stenosis and opportunities for pharmacologic intervention. Angiographic evaluation should be tailored to the type of systemic-to-pulmonary collateral artery anatomy found in each patient.
Roy, 38 years: A more in-depth discussion of control charts and their interpretation can be found in the Improvement Guide (18). For drugs with a narrow therapeutic index such as digoxin, the difference between the systemic exposure (plasma levels) associated with therapeutic and adverse effects is small. If too few subjects are studied the possibility of erroneous conclusions is increased; if too many subjects are studied there is greater cost and loss of efficiency. Other means to improve systemic perfusion include therapies that attenuate sympathetic vascular tone.