-
(786) 502-2173
-
We've gone mobile!
-
Hours: By Appointment Only
Only $0.37 per item
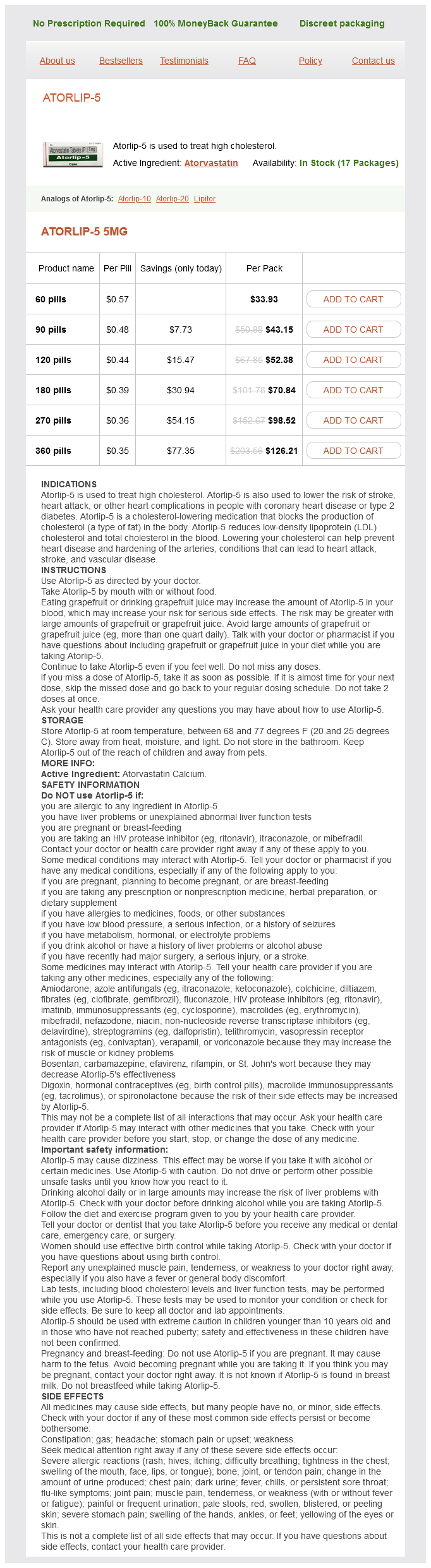
Atorlip-5 dosages: 5 mg
Atorlip-5 packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 841
Rituximab in a patient with multiple sclerosis-effect on B cells cholesterol levels numbers 5 mg atorlip-5 order visa, plasma cells and intrathecal IgG synthesis. Changes in B-and Tlymphocyte and chemokine levels with rituximab treatment in multiple sclerosis. Distinct effector cytokine profiles of memory and naive human B cell subsets and implication in multiple sclerosis. Ocrelizumab in relapsing-remitting multiple sclerosis: A phase 2, randomised, placebo-controlled, multicentre trial. Safety and efficacy of ofatumumab in relapsingremitting multiple sclerosis: A phase 2 study. Daclizumab (Zenapax) inhibits early interleukin-2 receptor signal transduction events. A role for interleukin-2 trans-presentation in dendritic cell-mediated T cell activation in humans, as revealed by daclizumab therapy. Mitoxantrone in progressive multiple sclerosis: A placebo-controlled, double-blind, randomised, multicentre trial. Evidence Report: the efficacy and safety of mitoxantrone (Novantrone) in the treatment of multiple sclerosis. Feasibility of cell therapy in multiple sclerosis: A systematic review of 83 studies. Clinical and pathological effects of intrathecal injection of mesenchymal stem cell-derived neural progenitors in an experimental model of multiple sclerosis. Safety and immunological effects of mesenchymal stem cell transplantation in patients with multiple sclerosis and amyotrophic lateral sclerosis. Bone marrow mesenchymal stem cell transplantation in patients with multiple sclerosis: A pilot study. Neural precursors attenuate autoimmune encephalomyelitis by peripheral immunosuppression. Human neural stem cells ameliorate autoimmune encephalomyelitis in non-human primates. The development of hematopoietic and mesenchymal stem cell transplantation as an effective treatment for multiple sclerosis. Hematopoietic stem cell transplantation for progressive multiple sclerosis: Failure of a total body irradiationbased conditioning regimen to prevent disease progression in patients with high disability scores. Autologous haematopoietic stem cell transplantation with an intermediate intensity conditioning regimen in multiple sclerosis: the Italian multi-centre experience. Autologous hematopoietic stem cell transplantation with reduced-intensity conditioning in multiple sclerosis.
Dillweed (Dill). Atorlip-5.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96472
The thalamus and multiple sclerosis: Modern views on pathologic cholesterol vitamin d best 5 mg atorlip-5, imaging, and clinical aspects. Cognitive impairment is associated with subcortical magnetic resonance imaging grey matter T2 hypointensity in multiple sclerosis. Deep grey matter "black T2" on 3 tesla magnetic resonance imaging correlates with disability in multiple sclerosis. Deep grey matter T2 hypo-intensity in patients with paediatric multiple sclerosis. Deep gray matter T2 hypointensity is present in patients with clinically isolated syndromes suggestive of multiple sclerosis. Increased iron accumulation occurs in the earliest stages of demyelinating disease: An ultra-high field susceptibility mapping study in Clinically Isolated Syndrome. Expression of the translocator protein of 18 kDa by microglia, macrophages and astrocytes based on immunohistochemical localization in abnormal human brain. The peripheral benzodiazepine binding site in the brain in multiple sclerosis: Quantitative in vivo imaging of microglia as a measure of disease activity. Focal damage to an axon may lead to Wallerian degeneration of the distal segment separated from the cell body, whereas the proximal axon segment may die because of the lack of connections to other neurons. Loss of neurons may induce a further loss of neurons that have lost their connections by retrograde or anterograde transneuronal degeneration and, as a consequence, may lead to degeneration of axons and neurons in areas distant from the primary site of the inflammatory lesion. Together with postcontrast T1-weighted scans, they provide objective information about subclinical disease activity, which occurs at a rate 5 to 10 times higher than the one that could be detected clinically. As noted for T2 lesions, contrast-enhancing lesions also show a relatively modest correlation with disability accumulation. Studies assessing the correlations between T1-hypointense lesion burden and disability provided conflicting results, since some of them found such a correlation to be higher than for T2 lesions, whereas others did not. Columns and error bars represent means and standard deviations of atrophy measures. Such abnormalities become more severe with increasing disease duration and neurological impairment. These metabolic abnormalities were related with the extent of T2 lesions and the severity of clinical impairment. Orange circles identify regions with a correspondence between the presence of T2-visible lesions and cortical atrophy. Cognitive impairment in multiple sclerosis is associated to different patterns of gray matter atrophy according to clinical phenotype. Images are colour coded for activation, and arrows show cut-off values from within-group analysis with a one-sample t test (t > 5). Whether such functional abnormalities confer a systematic vulnerability to disease progression or, conversely, protect against the onset of clinical deficits needs to be investigated. Diagnostic criteria for multiple sclerosis: 2010 Revisions to the McDonald criteria. Large, nonplateauing relationship between clinical disability and cerebral white matter lesion load in patients with multiple sclerosis.
However xanthomas cholesterol treatment cheap atorlip-5 5 mg otc, several case reports showed that aggressive regimens combining glucocorticoids and cyclophosphamide improved outcomes as compared with the almost consistently fatal outcome of the earliest reported cases. In one of the first retrospective cohort studies,6 43% of patients received with glucocorticoids alone and 81% of these had good outcomes. The remaining patients also received cyclophosphamide, and 81% achieved a similar good outcome. Why the former patients did not also receive cyclophosphamide likely represents an indication bias. These latter findings may suggest that patients whose disease was severe enough to justify the use of cyclophosphamide achieved a relatively good outcome, whereas those with a less severe disease can receive glucocorticoids alone. However, in a more recent cohort,19 85% of patients received a combination of glucocorticoids and cyclophosphamide; the mortality rate was 6% as compared with 17% in the former cohort. The identification of patient subgroups and predictors of mortality or neurological damage might thus help in deciding adequate treatment and its intensity for individual patients. Patients with focal neurological deficits, cognitive impairments, cerebral infarctions, and/or large-vessel involvements are at high risk of death. Imaging tests to find abnormal vessels on angiography show vasculopathy but are not specific for underlying causes and are not sufficiently sensitive-such vessels can be absent in biopsy-proven vasculitis. Biopsies are specific for inflammation but do not differentiate primary from secondary vasculitides and remain insensitive because the tests can be negative up to 50% of the time, especially when symptomatic inflammatory changes. Notably, severe and/ or prolonged arterial spasms can lead to stroke, with a transient deficit reported to occur in 16% to 54% of patients, being definitive in 7%. Cyclophosphamide should be added for patients with more severe disease, as judged by the treating physician, because of no consensual or validated definition of severe disease. Cyclophosphamide can be given continuously (2 mg/kg/d, orally) or intermittently, such as intravenous pulses of 15 mg/kg per day every 3 to 4 weeks. Once the condition has improved and achieved an equivalence of remission (no consensual or validated definitions for response to treatment or remission yet), usually after a maximum of 6 months, cyclophosphamide should be stopped and possibly switched to a less toxic maintenance therapy, with azathioprine, methotrexate, or mycophenolate mofetil, for at least 1 to 2 years, as for systemic vasculitides. For patients with ischemic strokes, alternative causes (carotid artery disease, atrial fibrillation, coronary source) should be searched. Conventional vascular risk factors, including high blood pressure, high cholesterol level, and diabetes, should be treated and antiplatelet agents (or occasionally anticoagulation agents, for example, for patients with antiphospholipid antibody-mediated stroke or vasculitis) used as appropriate. Other agents and biologics can be considered for patients with relapsing and/or refractory disease but with limited evidence, from isolated case reports only. Report of 8 new cases, review of the literature, and proposal for diagnostic criteria. Adult primary central nervous system vasculitis treatment and course: analysis of one hundred sixty-three patients.
Syndromes
Additional information:
Usage: gtt.
Tags: order 5 mg atorlip-5, buy atorlip-5 5 mg without prescription, cheap 5 mg atorlip-5 with visa, order atorlip-5 5 mg otc
Javier, 58 years: These models have been instrumental in the evaluation of the pathogenic potential of candidate disease-causing mutations. Acute myocardial infarction associated with high dose intravenous immunoglobulin infusion for autoimmune disorders.
Kalesch, 24 years: Proinflammatory cytokines promote glial heme oxygenase1 expression and mitochondrial iron deposition: Implications for multiple sclerosis. Cerebrovascular reactivity to acetazolamide and outcome in patients with symptomatic internal carotid or middle cerebral artery occlusion: a xenon-133 single photon emission computed tomotraphy study.
Cronos, 46 years: Increased expression of alpha-synuclein reduces neurotransmitter release by inhibiting synaptic vesicle reclustering after endocytosis. Social behavior phenotypes in fragile X syndrome, autism, and the Fmr1 knockout mouse: Theoretical comment on McNaughton et al.
Faesul, 22 years: It causes enormous impairments in normal day-to-day function that goes beyond pure intellectual deficits. Innate immunity triggers oligodendrocyte progenitor reactivity and confines damages to brain injuries.
Ayitos, 56 years: Long-term otucome of West syndrome: A study of adults with a history of infantile spasms. This can progress to include paraphasic errors, impoverished speech content, and impaired comprehension.
Gamal, 55 years: Short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms is defined as at least 20 attacks occurring one or more times per day for more than half the time consisting of unilateral stabbing or pulsating pain in the temporal, orbital, or supraorbital regions lasting 2 seconds to 10 minutes. Modafinil to treat fatigue in amyotrophic lateral sclerosis: An open label pilot study.
Hjalte, 30 years: Permanent bilateral sensory and neural hearing loss of children after neonatal intensive care because of extreme prematurity: A thirty-year study. The antisense oligonucleotide knockdown leads to the fish having truncated motor axons as well as defective branching of the motor axon.