-
(786) 502-2173
-
We've gone mobile!
-
Hours: By Appointment Only
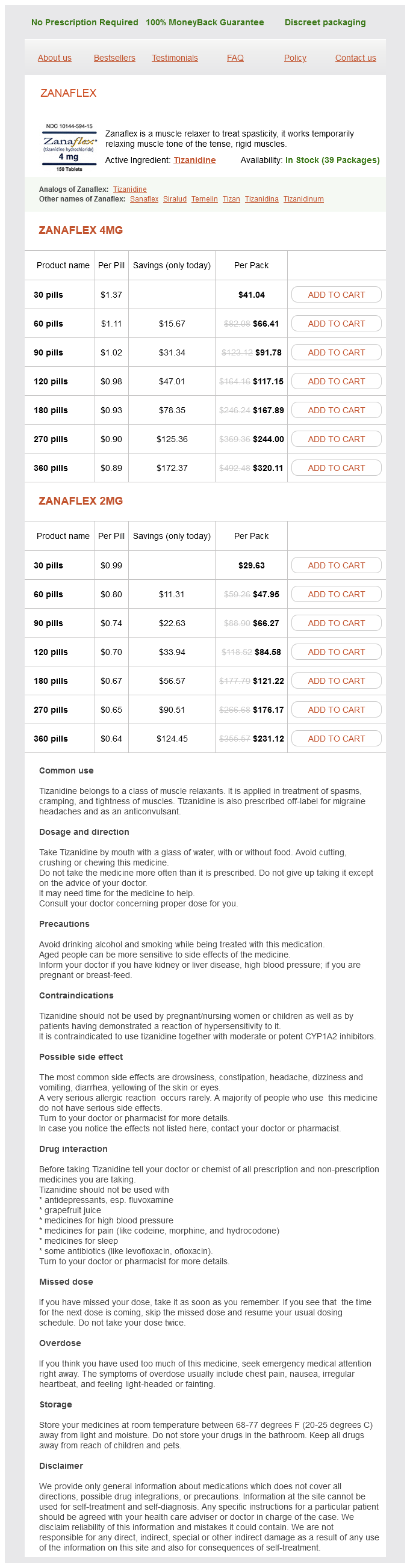
Only $0.64 per item
Zanaflex dosages: 4 mg, 2 mg
Zanaflex packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 554
Duodenal stump blowout results from progressive afferent limb dilation spasms stomach zanaflex 4 mg buy with amex, leading to peritonitis, abscess, or fistula formation. In the urgent setting, jejunojejunostomy can effectively decompress the afferent limb. A chronic form of afferent loop syndrome results from partial mechanical obstruction of the afferent limb. Patients present with postprandial right upper quadrant pain relieved by bilious emesis that is not mixed with recently ingested food. Stasis can lead to bacterial overgrowth and subsequent bile salt deconjugation in the obstructed loop, causing blind loop syndrome (steatorrhea and vitamin B12, folate, and iron deficiency) by interfering with fat and vitamin B12 absorption. Efferent loop syndrome results from intermittent obstruction of the efferent limb of the gastrojejunostomy. Patients complain of abdominal pain and bilious emesis months to years after surgery, similar to the situation with regard to a proximal small bowel obstruction. Postvagotomy diarrhea occurs in 20% after truncal vagotomy and is thought to result from alterations in gastric emptying and vagal denervation of the small bowel and biliary tree. Treatment includes antidiarrheal medications (loperamide, diphenoxylate with atropine, cholestyramine) and decreasing excessive intake of fluids or foods that contain lactose. A patient with gastric outlet obstruction and prolonged emesis has which electrolyte disturbance What is the preferred surgical therapy for hemodynamically unstable patients with bleeding duodenal ulcers Duodenotomy, three-point ligation of the bleeding vessels, highly selective vagotomy d. Duodenotomy, three-point ligation of the bleeding vessels, truncal vagotomy, pyloroplasty. Lymphadenectomy should be attempted given high propensity of lymph node metastasis c. Early gastric cancers always require total gastrectomy View Answer > Table of Contents > 18 - the Surgical Management of Obesity 18 the Surgical Management of Obesity Iheoma Nwaogu J. Christopher Eagon Obesity is a disease process that has reached epidemic proportions worldwide, with the highest prevalence in the United States, where 5% of the adult population is morbidly obese. Severe obesity is a condition characterized by the pathologic accumulation of excess body fat. The etiology of morbid obesity is poorly understood and thought to result from an imbalance in biologic, psychosocial, and environmental factors governing caloric intake and caloric expenditure. Risk factors for the development of morbid obesity include genetic predisposition, diet, and culture. Most patients with morbid obesity present with one or more of a number of weight-related comorbidities.
Hemlock Spruce. Zanaflex.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96451
Antimicrobial treatment should spasms synonym order zanaflex 4 mg on-line, however, be considered in patients with increasing cough, dyspnoea and increased production and purulence of sputum. Treatment Amoxicillin 500 mg orally every 8 hours for 5 days or amoxicillin 500 mg + clavulanic acid orally every 8 hours for 5 days or sulfamethoxazole 800 mg + trimethoprim 160 mg orally every 1224 hours for 5 days. Comments Chronic purulent bronchial infection and chronic airway disease are predominantly diseases of adults. Cystic fibrosis infections require specialist clinical management and laboratory services. Chronic recurrent cough Chronic cough is a common condition in adults and children associated with causes such as pollution, allergy, and passive and active smoking. The occurrence of a chronic cough with persistent fever and weight loss should raise clinical suspicion of tuberculosis or bronchial cancer. The respiratory rates above which pneumonia should be suspected are shown in the table overleaf. Other symptoms and signs of pneumonia include pleural pain, fever and crepitations. The etiology of pneumonia varies greatly with the age and geographical location of the patient. Pneumonia in adults and children aged over 5 years the most important pathogen in this age group is Streptococcus pneumoniae, followed by atypical bacteria such as Mycoplasma pneumoniae, Chlamydia pneumoniae, Legionella spp. Options for treatment of these infections have been considered by expert committees in many countries. The recommendations of these committees are based on the prevalence of resistance of S. Clinical presentation and Gram-staining of sputum may aid in the diagnosis of the etiological pathogen(s). Treatment Ambulatory patients Amoxicillin 500 mg (children: 15 mg/kg; maximum 500 mg) orally every 8 hours for 5 days or erythromycin 500 mg (children: 1015 mg/kg; maximum 500 mg) orally every 6 hours for 5 days (14 days in cases of atypical pneumonia) 22 Lower respiratory tract infections or doxycycline 100 mg (children > 8 years: 2 mg/kg; maximum 100 mg) orally every 12 hours for 710 days (contraindicated during pregnancy) or sulfamethoxazole 800 mg + trimethoprim 160 mg (children: 20 mg/kg + 4 mg/kg; maximum 800 mg + 160 mg) orally every 12 hours for 5 days. In cases of atypical pneumonia, treatment is as described above, with the addition of erythromycin 1 g (children: 10 mg/kg; maximum 1 g) i. Erythromycin should be used only in regions where the prevalence of resistance of S. Gentamicin is not recommended for patients with significant renal failure (creatinine clearance < 20 ml/min). Pneumonia in children aged from 2 months to 5 years In developing countries pneumonia in children aged from 2 months to 5 years is usually due to Streptococcus pneumoniae or Haemophilus influenzae or occasionally Staphylococcus aureus.
However spasms constipation buy 4 mg zanaflex free shipping, when the clinical picture and physical examination are sufficiently uncertain or in the unresponsive patient, compartment pressures should be measured. A difference between diastolic blood pressure and compartment pressure of <30 mm Hg is diagnostic of compartment syndrome (J Bone Joint Surg Br. Fasciotomy of all involved compartments is necessary when compartment syndrome is diagnosed. Prophylactic fasciotomy should also be performed after repair of traumatic vascular injuries (particularly those presenting with ischemia). A single incision should start 1 cm proximal and 2 cm lateral to the medial epicondyle, extend medially and obliquely across the antecubital fossa over the volar aspect of the brachioradialis muscle, and then turn distally and medially into the midline, where it is extended longitudinally just ulnar to the palmaris longus tendon. The incision should be curved across the wrist crease to allow for carpal tunnel release. An adequate fasciotomy of the forearm in the setting of trauma includes careful release of the lacertus fibrosus in the medial portion of the antecubital fossa, the fascia over the brachioradialis/mobile wad muscles laterally, the fascia of the superficial and deep extrinsic muscles of the forearm, and carpal tunnel release. Many times, the pressure in the dorsal compartment of the forearm is decreased following volar fasciotomy; however, if pressure remains elevated in the dorsal compartment, a second incision should be made from 2 cm distal to the lateral epicondyle extending distally toward the midline of the wrist (10 cm in length) to visualize and then release the fascia overlying the dorsal forearm muscles. The lateral incision should be made 1 cm anterior to and in line with the fibula, extending from the fibular head to 4 cm proximal to the lateral malleolus. The incision is taken through the skin and subcutaneous tissue to the level of the fascia. The subcutaneous flap is raised off the fascia medially in order to identify the intermuscular septum between the anterior and lateral compartments, through which perforating vessels to the skin are seen. Care must be taken to identify and protect the superficial peroneal nerve in the subcutaneous space crossing from lateral to medial at the distal portion of this fascial incision. Next, subcutaneous flaps are raised as needed to expose the fascia of the lateral compartment 1 cm lateral/posterior to the fibula. The fascia over the entire length of the wound must be incised to expose the muscular origins proximally and beyond the myotendinous junctions distally. The superficial peroneal nerve, located deep to the fascia of the lateral compartment at the mid-leg and superficial to the fascial just distal to the midleg and proximal to where it was identified over the anterior compartment, needs to be found and protected. The medial incision should be 1 to 2 cm posterior to the medial border of the tibia and extended from the level of the knee to the ankle. The greater saphenous vein and saphenous nerve in the subcutaneous tissue ought to be identified and retracted anteriorly for protection. Fascia should be incised from the gastrocnemius-soleus complex over the entire course of the wound. To visualize the fascia of the deep compartment adequately, it is necessary that a portion of the soleus origin on the posterior and proximal tibia be released. Care must be taken not to incise too far medially and risk injury to the posterior tibial artery and vein. Once the soleus origin has been elevated, the fascia over the flexor digitorum longus can be visualized and incised over the entire course of the wound. A single, straight incision should be made through the skin and subcutaneous tissue in line with the fibula from the fibular head to 4 cm proximal to the lateral malleolus.
Syndromes
Additional information:
Usage: p.o.
Tags: discount 2 mg zanaflex visa, buy zanaflex 2 mg online, generic zanaflex 4 mg buy on-line, 4 mg zanaflex order mastercard
Akrabor, 35 years: After several months of trying different antibiotics, my doctors told me they had nothing left to offer, and that I should say my goodbyes to my family. In areas endemic for the disease where the organism is not known, therapy should encompass all three possible pathogens.
Hamid, 53 years: Clinical information Uses Treatment of: · severe croup (laryngotracheobronchitis) in neonates · epiglottitis in neonates, together with rifampicin · neonatal pneumonia · osteomyelitis due to Haemophilus influenzae or unknown pathogen in neonates, together with cloxacillin and amoxicillin + clavulanic acid · osteomyelitis due to Salmonella spp. We are committed to an equitable educational system without disparities in access to affordable, culturally appropriate, and acceptable maternity care provider education for all communities.
Frithjof, 52 years: This analysis was unable to determine whether there were equally beneficial effects racial groups such as African Americans (N=41), or Asians (N=93) who were the minority of subjects compared to Whites (N=714). Students create a scatterplot that correctly represents the Variant X and Y frequency numbers for each generation, with symbols distinguishing each variant and a relevant scale, axis labels, unit labels, legend, and title.
Harek, 48 years: Surgical site infection is more commonly associated with treatment of open fractures and treatment of certain fracture types. Contraindications · Because of its unpredictable toxicity, chloramphenicol should never be used in diseases which are safely and effectively treated by other antimicrobials.
Yorik, 40 years: Both are growing economies, with limited resources and capacity particularly in rural areas, large population bases and increasing access to mobile phones. There were four rounds of chemotherapy over the next months, with brief home respites between rounds until April when she went into remission.
Sugut, 21 years: Calcitonin-gene-related peptide and substance P are two of many neuropeptides which may be important in modulating acid secretion. In addition, the prescribing physician must be conscious of these interactions so as to avoid errors that may provoke medicolegal action.
Gambal, 59 years: The purpose of this broader education base is not simply to yield a better understanding of differing practices, but primarily to promote the best care for patients by intelligently selecting the most facilitating route to health and wellness. It is caused by a rapid shift of extracellular fluid into the bowel lumen in response to a hyperosmolar load entering the small intestine from the stomach.