-
(786) 502-2173
-
We've gone mobile!
-
Hours: By Appointment Only
Only $0.26 per item
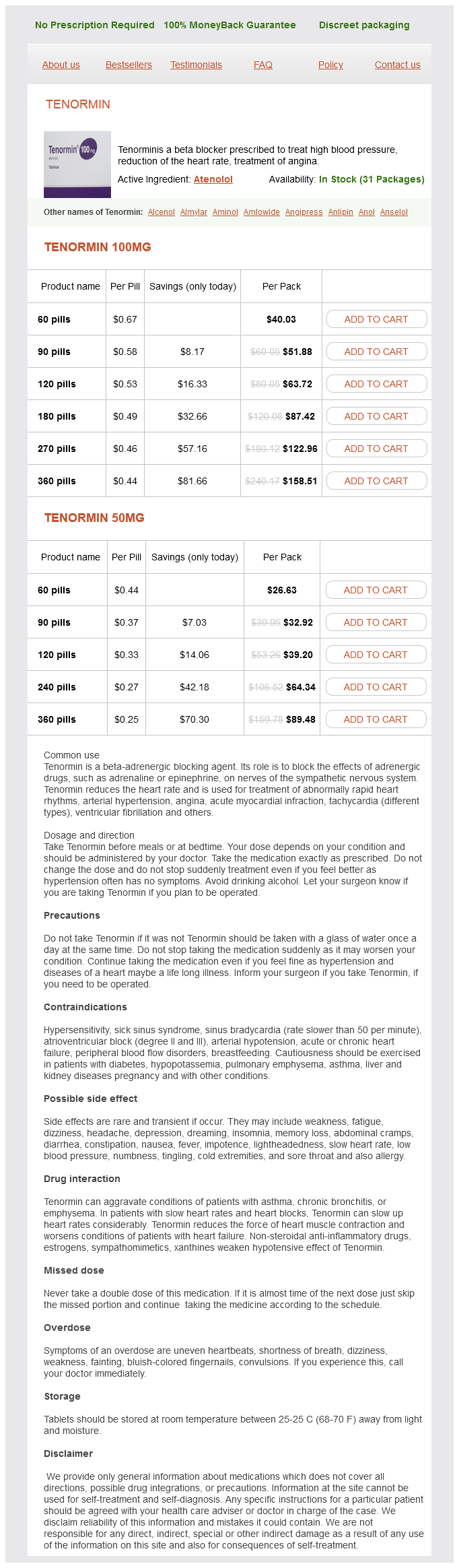
Tenormin dosages: 100 mg, 50 mg
Tenormin packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills, 240 pills
In stock: 721
Because of the limitations in sensitivity of currently available molecular assays arteria apendicular discount tenormin 50 mg without a prescription. Antibody neutralization limits intrahepatic spread of virus during primary infection and serves an important role in preventing reinfection. These consecutive phases are much more likely to be apparent in patients with acquisition of chronic hepatitis B early in life. The newer nomenclature is based on the description of the 2 main characteristics of chronicity: infection (no inflammation) versus hepatitis (inflammation). Whereas both cellular and humoral immune responses are needed for effective clearance and long-term protection against reinfection, the cellular immune response appears to be the arm principally involved in the pathogenesis of disease. The course is shown graphically in A, and the criteria for each phase are shown in B. If the patient has not entered this phase and is not treated, late disease complications often occur. The relative time dimensions of each phase are shown; note that there may be significant overlap of features among the various phases. If the active hepatitis phases remain untreated, cirrhosis can be anticipated to develop in at least 20% of cases. The disease may be more severe in patients coinfected with other hepatitis viruses and in those with established underlying liver disease. These features generally abate before the manifestations of liver disease and peak serum aminotransferase elevations are observed. Patients older than 40 years of age appear to be more susceptible than younger persons to "late-onset" liver failure, which occurs several months after the onset of acute symptoms and is associated with encephalopathy and renal dysfunction. When symptoms are present, fatigue tends to predominate over other constitutional symptoms, such as poor appetite and malaise. Cryoglobulinemia may be associated with systemic vasculitis (purpura, arthralgias, peripheral neuropathy, and glomerulonephritis) but is often asymptomatic. Nucleos(t)ide analog therapy has been used successfully to treat symptomatic cryoglobulinemia. They are important to recognize because they may occur without clinically apparent liver disease and can be mistaken for independent disease processes in other organ systems. The pathogenesis is not completely understood but likely involves an aberrant immunologic response to extrahepatic viral proteins. Serum complement levels are generally low, and antiviral therapy may be beneficial in reducing the amount of immunologically activating viral antigens. Plasmapheresis may be useful, but the best therapeutic responses have also been observed with antiviral agents, given alone or in combination with plasmapheresis or immunosuppressive therapy.
Blood of the Dragon (Sangre De Grado). Tenormin.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96737
These nonspecific symptoms are found with similar frequencies in persons without gallstones blood pressure yoga ramdev tenormin 50 mg order with visa. Physical findings are usually normal, with only mild to moderate gallbladder tenderness during an attack and perhaps mild residual tenderness lasting several days after an attack. Acute biliary pain improves with administration of meperidine, with or without ketorolac or diclofenac. In approximately 90% of cases, the underlying cause is obstruction of the outlet of the gallbladder by a gallstone in the cystic duct, gallbladder neck, or Hartmann pouch. Acute cholecystitis caused by gallstones is a disease of young, otherwise healthy women and generally has a favorable prognosis, whereas acute acalculous cholecystitis occurs more commonly in critically ill patients and is associated with high morbidity and mortality rates. Pathogenesis Acute cholecystitis generally occurs when a stone becomes embedded in the cystic duct and causes chronic obstruction, rather than transient obstruction as in biliary pain. In animal studies, if the cystic duct is ligated, the usual result is gradual absorption of the gallbladder contents without the development of inflammation292; the additional instillation of a luminal irritant. Phospholipase A is believed to be released by gallstone-induced mucosal trauma and converts lecithin to lysolecithin. Although normally absent from gallbladder bile, lysolecithin is present in the gallbladder contents of patients with acute cholecystitis. Studies of human tissue obtained at cholecystectomy have demonstrated enhanced prostaglandin production in the inflamed gallbladder. Elevations of serum bilirubin, alkaline phosphatase, or amylase levels suggest coexisting choledocholithiasis. Usually a carefully taken history assists in narrowing the differential diagnosis. These data suggest a chain of events in which obstruction of the cystic duct in association with 1 or more intraluminal factors damages the gallbladder mucosa and stimulates prostaglandin synthetase. The resulting fluid secretion and inflammatory changes promote a cycle of further mucosal damage and inflammation. Later in the attack, the bile pigments that are normally present are absorbed and replaced by thin mucoid fluid, pus, or blood. If the attack of acute cholecystitis is left untreated for a long period but the cystic duct remains obstructed, the lumen of the gallbladder may become distended with clear mucoid fluid, a condition known as hydrops of the gallbladder. Histologic changes range from mild acute inflammation with edema to necrosis and perforation of the gallbladder wall. One study has shown that acute cholecystitis resolves without complications in about 83% of patients but results in gangrenous cholecystitis in 7%, gallbladder empyema in 6%, perforation in 3%, and emphysematous cholecystitis in fewer than 1%. If biliary pain has been constant for more than 6 hours, acute cholecystitis should be suspected.
Although the ectoplasmic leaflet of the canalicular membrane is cholesteroland sphingomyelin-rich and is relatively resistant to penetration by bile salts heart attack sam tsui chrissy costanza of atc tenormin 50 mg mastercard, bile salts may promote vesicular secretion of biliary cholesterol and phosphatidylcholine. Bile salts may partition preferentially into these areas to destabilize the membrane and release phosphatidylcholine-rich vesicles because detergent-like bile salt molecules within the canalicular space could interact with the canalicular membrane. The relationship between bile salt secretion and cholesterol secretion is curvilinear: At low bile salt secretion rates (usually <10 mol/hr/kg), more cholesterol is secreted per molecule of bile salt than at higher rates. Although bile salt secretion rates are not low in normal subjects, they may diminish during prolonged fasting, during the overnight period, and with substantial bile salt losses, as occur with a biliary fistula or ileal resection when the liver cannot compensate sufficiently by increasing bile salt synthesis. At high bile salt secretion rates, for example, during and after eating, biliary cholesterol saturation is less than that during interprandial periods. In laboratory animals, biliary secretion of organic anions does not influence bile salt secretion but does inhibit hepatic secretion of phospholipids and cholesterol into bile because organic anions bind bile salts within bile canaliculi and prevent interactions with the canalicular membrane of hepatocytes. The hypothesis proposed is that hepatic hypersecretion of biliary cholesterol is the primary defect and is the outcome, in part, of a complex genetic predisposition. A major result of gallbladder hypomotility is alteration in the kinetics of the enterohepatic circulation of bile salts (intestinal factors). Alterations in intestinal factors result in increased cholesterol absorption, as well as reduced bile salt absorption, that leads to abnormal enterohepatic circulation of bile salts and a diminished biliary bile salt pool size. Not only does gallbladder hypomotility facilitate cholesterol nucleation and crystallization, but it also allows the gallbladder to retain solid plate-like cholesterol monohydrate crystals. Hepatic Hypersecretion of Biliary Cholesterol Hepatic hypersecretion of biliary cholesterol plays a primary role in the pathogenesis of cholesterol gallstone formation. By definition, supersaturated bile contains cholesterol that cannot be solubilized at equilibrium by bile salts and phospholipids. Cholesterol supersaturation could result from (1) excessive hepatic secretion of biliary cholesterol, (2) decreased hepatic secretion of biliary bile salts or phospholipids with relatively normal cholesterol secretion, or (3) a combination of hypersecretion of cholesterol and hyposecretion of the solubilizing lipids. With the passage of time and in the presence of heterogeneous pronucleating agents (usually mucin gel), cholesterol supersaturation leads to precipitation of solid plate-like cholesterol monohydrate crystals in bile, followed by agglomeration and growth of the crystals into mature and macroscopic stones. Rapid Cholesterol Nucleation and Crystallization Cholesterol nucleation and crystallization is a process by which solid plate-like cholesterol monohydrate crystals precipitate from supersaturated bile. The crystals can be detected by polarizing light microscopy in a sample of bile previously rendered crystal-free ("isotropic"). On the other hand, rapid in vitro cholesterol nucleation and crystallization from the isotropic phase of gallbladder bile distinguishes the lithogenic bile of patients with cholesterol gallstones from cholesterol-supersaturated bile of nongallstone control subjects. In these pathways, the critical nucleus may be a unilamellar vesicle that could contain liquid anhydrous cholesterol molecules in its core, possibly reflecting internal nucleation. In essence, these early vesicular "nuclei" may already have initiated the nucleation cascade by the time bile enters the gallbladder. The current paradigm for cholesterol nucleation and crystallization, based principally on observations from video-enhanced polarized light microscopy, suggests that biliary vesicles must fuse or at least aggregate to form crystalline cholesterol monohydrate. Because cholesterol nucleation and crystallization are apparently initiated in vesicles, the stability of the vesicle determines the stability of bile. Unstable vesicles can fuse, aggregate, and grow into multilamellar liquid crystalline structures (liposomes) in which cholesterol crystallizes out of solution.
Syndromes
Additional information:
Usage: q.3h.
Tags: best 100 mg tenormin, buy tenormin 100 mg on-line, buy generic tenormin 100 mg online, 100 mg tenormin order fast delivery
Ortega, 40 years: In the early stages within the pancreas, chronic inflammation, cellular necrosis and apoptosis, and activation of pancreatic stellate cells have all developed, but these features of chronic pancreatitis remain visible only on histology. Measuring fecal fat requires that the dietary content of fat be known exactly, which is difficult to ascertain.
Trano, 23 years: The progression of disease is variable but ultimately results in cirrhosis and hepatic failure in a high proportion of affected persons. Gallbladder Dysfunction Under normal physiologic conditions, frequent gallbladder contractions occur throughout the day.
Ramon, 62 years: Erosive Disease Patients with erosive esophagitis tend to be male, older, and overweight and are more likely to have hiatal hernias. The role of actin filaments and microtubules in hepatocyte spheroid self-assembly.