-
(786) 502-2173
-
We've gone mobile!
-
Hours: By Appointment Only
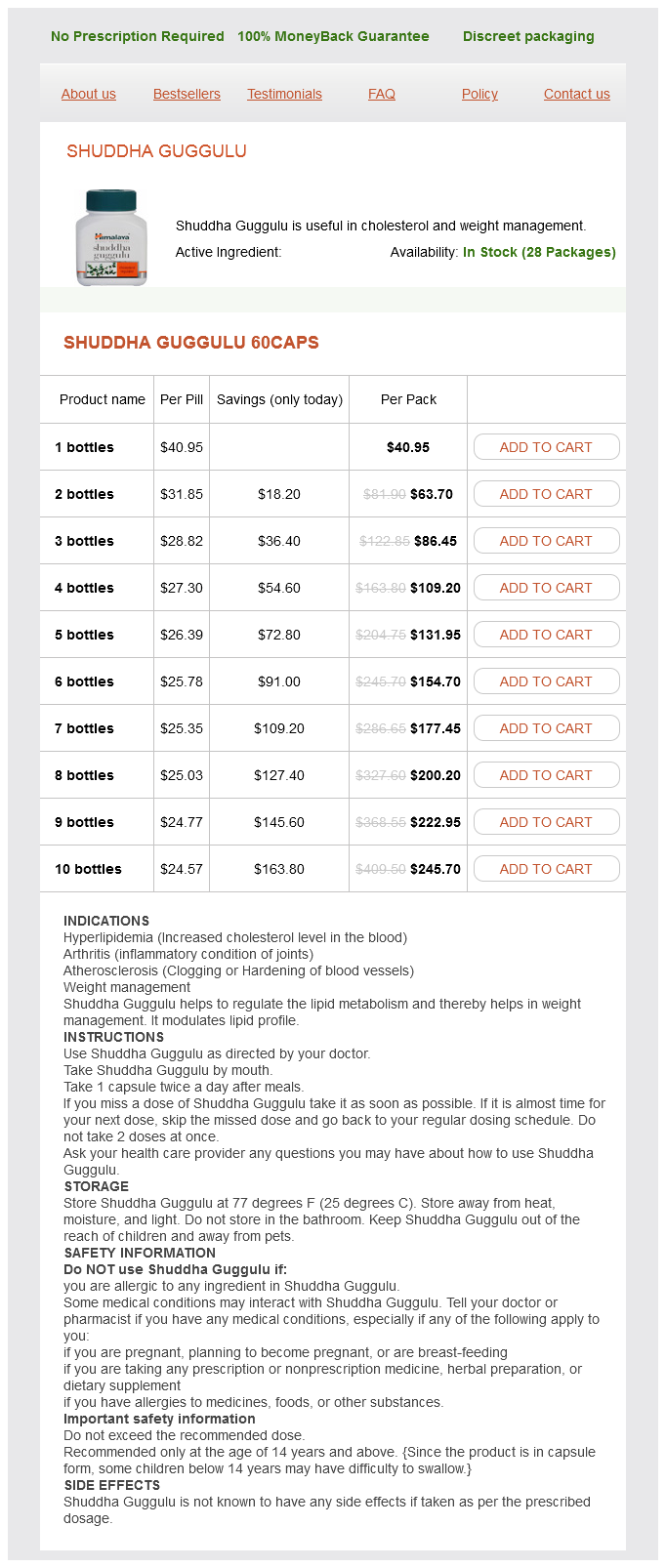
Only $26.11 per item
Shuddha Guggulu dosages: 60 caps
Shuddha Guggulu packs: 1 bottles, 2 bottles, 3 bottles, 4 bottles, 5 bottles, 6 bottles, 7 bottles, 8 bottles, 9 bottles, 10 bottles
In stock: 902
More recent investigations have shown an increased sensitivity of nerve cells close to the level of injury weight loss xls cheap 60 caps shuddha guggulu with visa. These nerve cells have a higher amount of background activity, greater amount of responsiveness to stimuli, and a longer duration of firing. Additional changes are suggested to occur at the molecular level and include changes to the level and function of neurotransmitters and their receptors. Glial activation occurs following injury, leading to increased secretion of prostaglandins and various cytokines. Structural changes are known to occur, with restructuring of connections in the dorsal horn. More recent work has focused on thalamocortical dysrhythmia and the plasticity and reorganizational changes that occur in the brain. The methods of treating neuropathic pain are broad, but principles center around treating the underlying causes of pain. Surgical options should always focus first on decompressing nervous tissue, untethering the spinal cord, or dealing with a syrinx formation. If these measures do not provide a satisfactory remedy to the pain, then disconnecting the site of abnormal activity is the next appropriate step. Lesions in the dorsal root entry zone can be used to destroy an area of hyperactive nerve cells in the dorsal horn cells in close proximity to the level of the injury. Most studies suggest that 50% to 85% of patients have a good amount of relief of pain from this procedure (Siddall, 2009). Electrophysiological techniques such as intramedullary recording of C-fiber evoked electrical hyperactivity may aid in targeting the lesion. Local and parenteral administration of lidocaine has been shown to be beneficial in treating neuropathic pain, but local administration is generally not long-lasting, and parenteral administration is typically impractical. Opioids, antiepileptics, and antidepressants increase inhibitory signals and limit excitability of neurons transmitting pain signals. Two randomized controlled studies show improvement of neuropathic pain following administration of parenteral morphine (Attal et al. Current recommendations for pharmacological treatment are directed at symptomatic relief and include first-line agents such as systemic lidocaine, gabapentin, and pregabalin. Although a recent randomized study failed to show benefit from the use of gabapentin in treating neuropathic pain (Rintala et al. Other new agents that may be considered include lamotrigine and topiramate; topiramate in particular has had encouraging results (Harden et al. In patients with localized symptoms, topical lidocaine therapy may provide relief. Intrathecal morphine and clonidine has provided short-term pain relief by acting on the opioid receptors of the dorsal horn of the spinal cord.
Glicerol (Glycerol). Shuddha Guggulu.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96054
IntraventricularHemorrhage Extension of hemorrhage into the ventricular system is a common feature of caudate and thalamic hemorrhages and of large putaminal and lobar hemorrhages weight loss unintentional shuddha guggulu 60 caps purchase fast delivery. The site of origin of the hemorrhage is thought to be the vasculature of the subependymal region, and rarely the source can be identified in the choroid plexus. Those from aneurysm rupture are generally due to an anterior communicating artery aneurysm that ruptures in an upward direction, bleeding directly into one of the lateral ventricles; in these instances, basal frontal subarachnoid hemorrhage and interhemispheric hemorrhage accompany the intraventricular hemorrhage and should always suggest a ruptured aneurysm. The clinical presentation of intraventricular hemorrhage is with acute onset of headache, nausea, vomiting, and decreased level of consciousness, with focal neurological deficits either minimal or altogether absent (Flint et al. Even after extensive testing, the cause of many intraventricular hemorrhages remains unknown. The prognosis of intraventricular hemorrhage is strongly dependent on the severity of the initial manifestation and its mechanism. Patients who are comatose as a result of the initial hemorrhage generally succumb, especially if they have early signs of brainstem involvement (ophthalmoparesis, loss of pupillary reflexes, decerebrate rigidity). Those who remain alert or obtunded without signs of parenchymal involvement tend to recover without neurological sequelae, although memory disturbances may be a relatively frequent residual deficit (Flint et al. Patients with the idiopathic form of intraventricular hemorrhage have the best prognosis. If the patient has a depressed level of consciousness and a Glasgow Coma Scale score of 8 or less, endotracheal intubation should follow. Coagulation studies are essential, especially in instances of hemorrhage in patients receiving anticoagulants, those previously treated with thrombolytic agents, or patients with liver disease. Coagulation abnormalities in patients receiving anticoagulants should be treated emergently because if anticoagulation is not reversed, it can lead to progressive enlargement of the hematoma. Activated charcoal may also be used to reduce the absorption of recently ingested capsules. Although dexamethasone is frequently given with the purpose of decreasing intracranial hypertension by reducing cerebral edema, its use is not supported by data from a single controlled clinical trial (Broderick et al. However, this potential benefit of antihypertensive therapy must be balanced against the possible harmful effects of drug-induced hypotension, with resulting cerebral ischemia and further neurological deterioration. In cases presenting with systolic blood pressure between 150 and 220 mm Hg, further reduction of systolic blood pressure to 140 mm Hg is safe and may improve clinical outcome (Anderson et al. In patients who did not have early seizures, there is a negligible risk of late epilepsy. Few scientific data are available to assist the clinician in this therapeutic choice.
Chronic syndromes have been treated successfully with a variety of drugs including the tetracycline demeclocycline weight loss 7-day water fast purchase 60 caps shuddha guggulu with mastercard, which interferes with the action of antidiuretic hormone on the renal tubules. In these patients, fluid restriction may lead to further volume reduction and cerebral infarcts during the period of the highest risk for vasospasm. The mechanisms underlying this phenomenon are unclear but may be related to the complexity of the peptidergic neurotransmitter systems in the vicinity of the third ventricle and to the possibility that they are damaged by the ruptured aneurysm. Damage is especially likely with an aneurysm on the anterior communicating artery. Hyponatremia occurs in approximately 1% of patients with recent surgical procedures. Because the symptoms are frequently mild or attributed to the surgery itself, this diagnosis may be missed. Typically, these patients seem to do well in the immediate postoperative period and then develop symptoms and signs of encephalopathy. Men and postmenopausal women are less likely to develop postoperative hyponatremia than women who are still menstruating. Complications such as respiratory arrest are particularly likely to occur more frequently in menstruating women than in men or menopausal women. Thus, it is important to be particularly vigilant when evaluating younger women with postoperative encephalopathy. The signs and symptoms of deranged osmolality depend on the severity of the disturbance and the length of time elapsed between onset and clinical presentation. Typical complaints are nonspecific and include malaise, nausea, and lethargy, leading to obtundation and coma. Headache, due to brain swelling, and epileptic seizures may be encountered in patients with hyponatremia, especially in patients with an acute alteration of serum sodium levels. Although serum sodium levels below 120 mmol/L are considered serious, patients who develop this level of hyponatremia as a side effect of diuretics or antiepileptic treatment over a long period of time may present with only minor, if any, symptoms. Minor symptoms include dizziness, cognitive dysfunction, gait disturbances, and falls. However, patients in whom serum sodium levels decrease within a short time interval due to an acute overload of total body water are prone to develop brain edema, alterations of consciousness, and seizures. Children and young women are particularly vulnerable to hyponatremic brain damage. Of note is that brain adaptation to low serum sodium levels increases the risk of osmotic demyelination after rapid resolution of hyponatremia. The treatment of hyponatremia has always been controversial and has become more so since the link between hyponatremia treatment and the subsequent development of central pontine myelinolysis was recognized and experimental replication of the syndrome achieved. Investigators in one study were unable to identify the rate at which serum sodium concentration was corrected, the absolute magnitude of the correction, or the type of solution infused as a factor that predisposed to the development of central pontine myelinolysis. They noted that undoubtedly thousands of patients with symptomatic hyponatremia have been treated successfully using a large number of protocols, but these cases have not been reported.
Syndromes
Additional information:
Usage: ut dict.
Tags: purchase shuddha guggulu 60 caps with amex, buy 60 caps shuddha guggulu fast delivery, purchase 60 caps shuddha guggulu visa, shuddha guggulu 60 caps order on line
Fraser, 36 years: In the patient with enlarging ventricles who reaches an early plateau or declines in mobility and cognition, a diagnosis of symptomatic normalor high-pressure hydrocephalus must be considered. However, isolated drop attacks are seldom a manifestation of vertebrobasilar occlusive disease.
Nerusul, 61 years: Patients who had progressing deficit in the first hour of observation were excluded from the study because of the prevailing belief at that time that stroke in evolution should be anticoagulated. High-dose chemotherapy with stem cell rescue as initial therapy for anaplastic oligodendroglioma.
Dudley, 29 years: LaboratoryStudies the diagnosis is not difficult when the appropriate neurological syndrome and a low serum vitamin E level are both present. A small subset involving severe angulation or disruption of the C2C3 disk complex requires consideration of surgical stabilization as a primary treatment option.