-
(786) 502-2173
-
We've gone mobile!
-
Hours: By Appointment Only
Only $0.32 per item
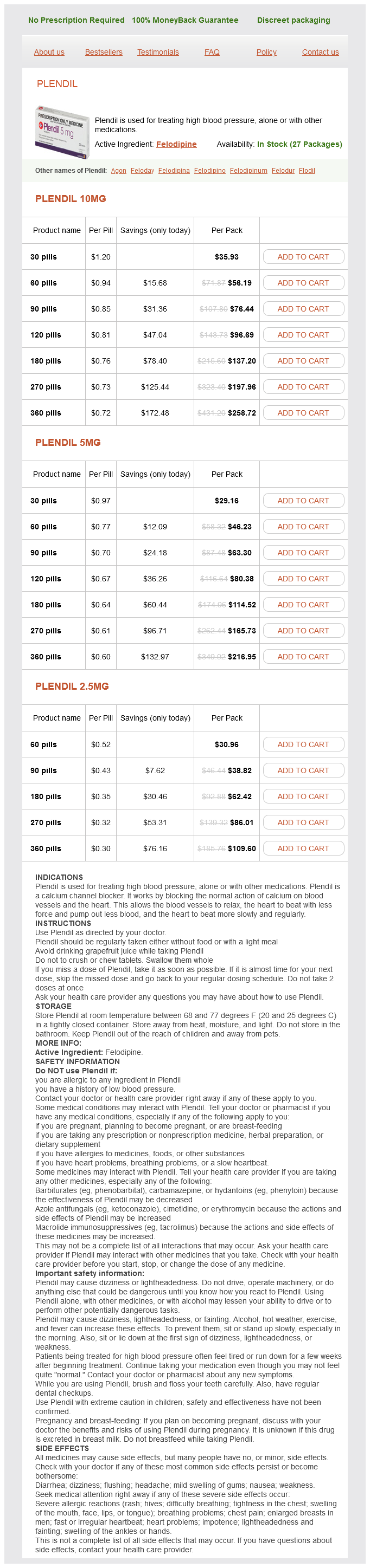
Plendil dosages: 10 mg, 5 mg, 2.5 mg
Plendil packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 853
Microscopically blood pressure ranges female plendil 2.5 mg low cost, early lesions contain polymorphonuclear (neutrophilic) leukocytic infiltrate in the marrow. Prominent formation of new reactive bone can be a dominant feature in later phases of the disease. Peculiar granulomas made up of collections of neutrophils surrounded by a rim of epithelioid histiocytes can be present, but there is no caseous necrosis. Results of bacterial, viral, and fungal cultures, as well as special stains for infectious organisms, are consistently negative. Some patients may have associated recurrent skin lesions (pustolosis palmoplantaris). In fact, it is postulated that chronic recurrent multifocal osteomyelitis is a manifestation of the spectrum of disorders characterized by sterile neutrophilic infiltrate primarily in the skin referred to as neutrophilic dermatoses. They include palmoplantar pustulosis, psoriasis, acne fulminans, neutrophilic eccrine hidradenitis, acute febrile netrophilic dermatosis, and pyoderma gangrenosum. Marginal erosions of tarsal bones and metatarsals are sharply outlined and completely radiolucent (arrows). Microscopic Findings Microscopically, monosodium urate crystals are needle shaped and demonstrate strongly negative birefringence under compensated polarization microscopy. Monosodium urate crystals are also found in tophi, where they form multicentric, radially oriented deposits surrounded by a matrix of amorphous material, lipids, and proteinaceous debris. A and B, Anteroposterior and lateral views of knee of patient with longstanding gout show bone erosion by tophaceous deposits of monosodium urate (arrows). Note radiolucent defects with sclerotic borders in femoral condyle, tibial plateau, patella, and fibular head. Clinical outcome of patients with chronic recurrent multifocal osteomyelitis is generally good, but some patients may have persistent disease after a long follow-up. Biopsy of the lesions is performed to confirm the inflammatory nature of the process, and the lesions are rarely confused with a nonhematologic neoplasm. However, the late phases of the process, characterized by the predominant lymphoid infiltrate, can be confused with lymphoma of the bone. It is helpful to consider in the differential diagnosis the entire clinical picture and radiographic presentation of the lesion. Lymphoma of the bone almost never occurs in young patients whose disease presents with multifocal involvement of metaphyseal parts. On the other hand, a destructive (permeative) lesion that occurs in a patient older than age 40 years and that is shown under a microscope to contain lymphoid cells is very unlikely to represent chronic osteomyelitis. Primary amyloidosis, with no associated generalized disorder, is very rare in the skeleton. The most frequent form of amyloidosis involving the skeleton is associated with multiple myeloma. It can affect the skeleton diffusely as a part of disseminated multiorgan disorder.
Lycium Barbarum (Lycium). Plendil.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96984
Percutaneous injection of calcitonin blood pressure chart in pediatrics proven plendil 5 mg, methylprednisolone, and sclerosing agents such as Ethibloc have been reported to be effective in inducing shrinkage and healing. Rare cases of high-grade sarcoma (osteosarcoma and malignant fibrous histiocytoma) developing at the site of a previously treated aneurysmal bone cyst have been described. Examples of spontaneous malignant transformation without previous radiation therapy also have been described. The prognosis and behavior of these lesions are generally determined by the biologic potential of the underlying condition. Incidence and Location More than 50% of all aneurysmal bone cysts are superimposed on a recognizable precursor condition. Both variants of aneurysmal bone cyst are rare in patients older than age 30 years. This indicates that young individuals, especially those who are skeletally immature, are more likely to develop this process, either as a primary or secondary phenomenon, compared with older individuals. On the other hand, there is no difference in predilection of primary versus secondary aneurysmal bone cyst in nonweight-bearing sites. Quite frequently, the underlying condition can be identified only microscopically. Because of the anatomic location, involvement of specific areas of bone, the age of the patient, and other factors, certain preexisting conditions can be anticipated. Chondroblastoma is almost invariably a source of a blowout lesion that develops in the calcaneus. It also should be suspected in the differential diagnosis of blowout lesions of the acetabulum. In skeletally mature patients, giant cell tumor is the frequent underlying condition of the blowout lesion in the end of long bones, especially if it involves the knee area. A, Blowout lesion of proximal humeral end represents secondary aneurysmal bone cyst superimposed on chondroblastoma. B, Expansile lytic lesion of intertrochanteric region of femur represents secondary aneurysmal bone cyst superimposed on nonossifying fibroma. C, Expansile lesion involves distal end of second metacarpal bone and is secondary aneurysmal bone cyst superimposed on giant cell reparative granuloma. A, Bisected rib with large secondary aneurysmal bone cyst engrafted on fibrous dysplasia. B, Specimen radiograph of A shows ground-glass appearance of more solid area at top, which contains fibrous dysplasia, and lucent area of aneurysmal bone cyst below. C, Radiograph of chondroblastoma of glenoid region of scapula with superimposed aneurysmal bone cyst. D, Low power photomicrograph of curetted material from C shows thickened septum of aneurysmal bone cyst with focus of chondroid matrix and sheets of chondroblasts.
The diagnosis of rare cases of chondrosarcoma distal to wrist and ankle joints is based on strict correlation between the radiographic and pathologic data blood pressure up heart rate down purchase 5 mg plendil mastercard. Treatment and Behavior the successful eradication of a malignant cartilage tumor depends on complete wide excision, if this is technically feasible. Other modalities, such as irradiation and chemotherapy, play a minor role and only apply to high-grade chondrosarcomas. Consequently the lesions located in anatomic sites where wide local excision is technically possible have better prognoses than those located at sites where complete removal is not possible. The overall prognosis is related to the size of the lesion, anatomic location, and histologic grade. Anderson Cancer Center indicate that the survival rate is strictly related to the histologic grade of the tumor,31 with 5-year survival rates of 90% for grade 1, 81% for grade 2, and 29% for grade 3 tumors. It is evident that the most significant difference in clinical behavior is between grade 2 and 3 chondrosarcomas. Recurrences in chondrosarcoma typically occur 5 to 10 years or more after surgery. In some instances, recurrence can be associated with an increase in histologic grade and more aggressive clinical behavior than that of the primary neoplasm. Chondrosarcoma metastasizes to the lymph nodes more frequently than other bone sarcomas. Grade 1 chondrosarcomas do not metastasize, but a fatal outcome in 10% of cases results from local uncontrollable growth. In addition, in rare cases, low-grade chondrosarcoma can recur as a highgrade pleomorphic (dedifferentiated) neoplasm. Although remote, the possibility of dedifferentiation should be considered if conservative management of a cartilage lesion is planned. Tumors that are not amenable to complete excision because of their location, such as the skull base, are treated by conventional radiotherapy for limited local control in the postoperative setting or in advanced inoperable cases with definitive intent. The use of proton therapy after maximal surgical resection in such locations offers increased probability of a long-term cure with relatively low risk of significant complications. The presence of radiologic changes in the adjacent cortex and surrounding cancellous bone and the clinical history regarding the events that led to the discovery of the cartilage lesion are of paramount importance in the recognition of a low-grade chondrosarcoma. A, Lateral radiograph of foot shows radiodense, heavily calcified chondrosarcoma in medullary cavity of calcaneus. B, Sagittally cut specimen from below-knee amputation shows grade 1 chondrosarcoma of calcaneus with extension into soft tissue. Note ivory-like areas corresponding to zones of enchondral ossification in hyaline cartilage of tumor. A and B, Frontal and oblique radiographs of chondrosarcoma involving proximal phalanx in third finger of a 72-year-old man. Tumor has ill-defined margins, permeative growth pattern, and matrix calcification.
Syndromes
Additional information:
Usage: q._h.
Tags: 10 mg plendil order fast delivery, buy 5 mg plendil with amex, discount 5 mg plendil fast delivery, 5 mg plendil order with amex
Mason, 31 years: A, Low power photomicrograph showing large areas of cartilaginous differentiation in peripheral parts of the tumor. Epidermal inclusion inclusion cysts typically occur in the acral skeleton and primarily involve the phalanges. We now understand that these tumors are not derived from macrophage-monocyte precursors.
Falk, 32 years: Suresh S, Muthukumar T, Saifuddin A: Classical and unusual imaging appearances of melorheostosis. Areas of immature reactive osteoid with prominent plump osteoblasts often raise the suspicion of a malignant, bone-forming tumor. The wall is composed of a paper-thin, tan-yellow fibrous tissue with multiple bony ridges.
Candela, 24 years: Well, immunologists have made rough estimates that about 100 million should do the trick. Briccoli A, Rocca M, Salone M, et al: High grade osteosarcoma of the extremities metastatic to the lung: long-term results in 323 patients treated combining surgery and chemotherapy, 19852005. Akai M, Tateishi A, Machinami R, et al: Chondroblastoma of the sacrum: a case report.
Marlo, 57 years: A and B, Anteroposterior and lateral radiographs of eccentric lytic lesion in proximal tibial metaphysis of female adolescent. In addition, the mentioned giant cellcontaining areas are typically focal, and the remaining material shows the bland-looking fibrous membrane of a solitary bone cyst. A, A T2-weighted coronal image through the penis and scrotum shows the paired dorsal corpora cavernosa (asterisks) surrounded by the hypointense tunica albuginea (arrows).
Charles, 51 years: Patient was clinically asymptomatic 2 years after second curettage and bone grafting. D, Higher magnification of C showing clusters of small neuroblastic cells adjacent to areas of solid proliferations of epithelioidappearing cells. A, Anteroposterior radiograph showing a metastatic pulmonary adenocarcinoma resulting in a large radiolucent defect in the humerus with cortical destruction and soft tissue extension.
Yasmin, 44 years: Enchondromatosis more frequently involves the small bones of the hands and also shows a more pronounced unilateral predominance than fibrous dysplasia. Essentially a transitional meningioma in which a large percentage of the meningothelial cell whorls have calcified (formed psammoma bodies). From the functional point of view, the intron D splicing-recognition sequence acts as a negative regulatory element by suppressing gene expression and presumably protecting the cell from the eventual transforming activity of the mutated (altered) gene product.