-
(786) 502-2173
-
We've gone mobile!
-
Hours: By Appointment Only
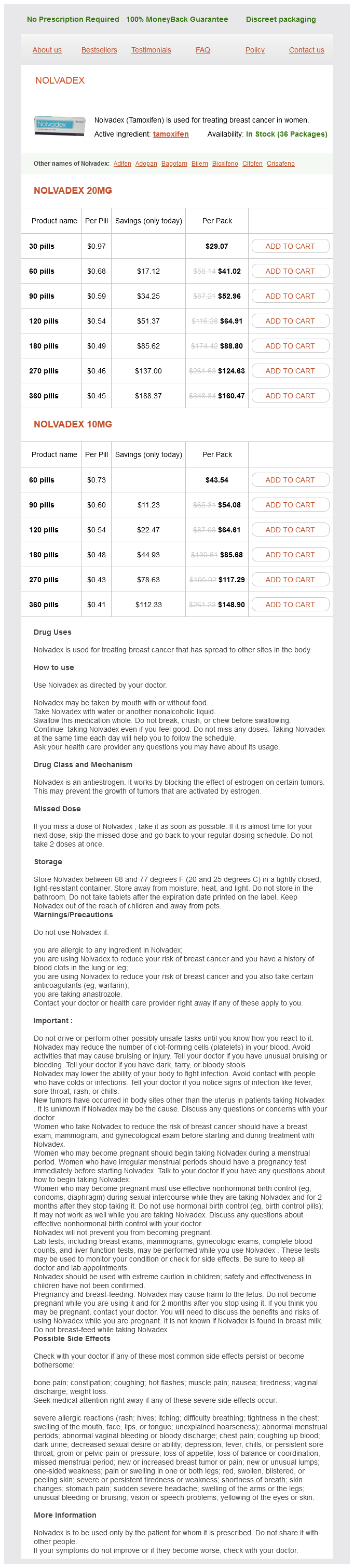
Only $0.44 per item
Nolvadex dosages: 20 mg, 10 mg
Nolvadex packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 999
Infants are rarely affected; lesions resolved after the use of oral tranilast and topical pimecrolimus in one such infant pregnancy 2 nolvadex 10 mg cheap. In the latter region, there is a lymphocytic and histiocytic dermal infiltrate that is distributed between collagen bundles. The infiltrate includes multinucleate giant cells, some of which contain asteroid bodies. There is variable loss of elastic fibers; it is complete in late stages of the disease. Therefore, granulomatous dermatoses should be examined carefully to exclude other etiologies. Polarization microscopy and special staining for organisms may be part of this evaluation. Two significant considerations in the differential diagnosis are granuloma annulare and necrobiosis lipoidica. This distinction is often possible because, unlike granuloma annulare and necrobiosis lipoidica, necrobiosis is not usually seen in annular elastolytic giant cell granuloma. The absence of increased dermal mucin also distinguishes most cases from granuloma annulare. In one study comparing actinic granuloma and granuloma annulare, the absence of elastotic material in the center of the lesions and the presence of scarring and giant cells with up to 12 nuclei were characteristic of actinic granuloma. By comparison, granuloma annulare was characterized by moderate amounts of elastotic material within granulomas, scarring was absent, and giant cells contained fewer nuclei. Histopathology the zonal histology described in actinic granuloma is also seen in this condition (discussed previously). There is destruction of dermal elastic tissue, with mild fibrosis in the center of annular lesions. In the raised active edge of the lesion, there is a granulomatous reaction that includes histiocytes, multinucleate giant cells, lymphocytes, eosinophils, and plasma cells. Areas of necrobiosis have been described, surrounded by a palisaded rim of histiocytes, in the middle and upper dermis in the annular rim. Phagocytosis of ochronotic fibers is seen, with these fibers representing pigmented swollen collagen fibers. There may be epidermal changes associated with transepidermal elimination of ochronotic material in this region. The central zone has an atrophic epidermis with underlying absence of elastotic material and ochronotic fibers together with mild fibrosis. There are a variety of reports of suppurative granulomas with organisms, foreign body granulomas with and without organisms, and caseation necrosis. This pattern was said to be a clue to an immunodeficiency that took the form of agammaglobulinemia.
Dolichos hirsutus (Kudzu). Nolvadex.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96732
Phenylketonuria women's health center towson md discount nolvadex 10 mg buy line, an autosomal recessive disorder with a deficiency of the enzyme L-phenylalanine hydroxylase, is characterized by oculocutaneous pigmentary dilution in addition to neurological abnormalities. Destruction of melanocytes: vitiligo, VogtKoyanagiHarada syndrome, chemical leukoderma 3. Sometimes a small number of morphologically abnormal melanocytes are present, particularly near the margins of hypopigmentation. Some clear cells, representing Langerhans cells, are usually present in the epidermis. It can occur in three different settings: limited to mucosa, initial involvement of mucosa later spreading to the skin, and cutaneous vitiligo spreading to mucosa (the latter being the most common circumstance in one study). In approximately 20% of cases, it develops after severe sunburn or some severe emotional or physical stress. The evolution and therapeutic monitoring of vitiligo can be carried out using in vivo reflectance confocal microscopy. It has been proposed that the segmental form (type B) of vitiligo results from dysfunction of sympathetic nerves in the affected areas. It is assumed that affected individuals have an intrinsic inability to eliminate or handle these toxic precursors, such as free radicals, which accumulate and result in the destruction of melanocytes by apoptosis. A melanocyte with a giant melanosome is present at the edge of the depigmented area. However, sampling of a lesion that includes the lesional border might show mild melanocyte enlargement, spongiosis, or interface changes features that would be more in keeping with vitiligo. Depigmentation accompanying certain inflammatory diseases, such as discoid lupus erythematosus, may also show characteristic epidermal, appendageal, or inflammatory changes, whereas scarring in a depigmented area suggests the effects of either a prior inflammatory process or trauma, such as a burn or radiation injury. Molecular studies have found that some lesions of vitiligo show focal melanocyte survival. In 16% of cases, there was some melanin in the basal layer with the MassonFontana stain. Ocular disorders include photophobia, nystagmus, strabismus, and reduced visual acuity. In the skin, there is accelerated photoaging and an increased incidence of keratoses and squamous and basal cell carcinomas. Lipid and ceroid pigment are present in macrophages in various organs, including the skin. It includes immunodeficiency in its phenotype, and patients have an increased susceptibility to infections as a consequence of neutropenia.
Giant cell (temporal) arteritis: Involvement of the vertebral and internal carotid arteries obama women's health issues 20 mg nolvadex purchase fast delivery. Association of temporal arteritis, retinal vasculitis, and xanthomatosis with multiple myeloma: Case report and literature review. Temporal arteritis presenting with scalp necrosis and a normal erythrocyte sedimentation rate. Scalp necrosis in temporal (giant cell) arteritis: Implications for the dermatologic surgeon. Magnetic resonance angiography in the diagnosis of a case of giant cell arteritis manifesting as scalp necrosis. Actinic granuloma in association with giant cell arteritis: Are both caused by sunlight Annular elastolytic giant cell granuloma associated with temporal arteritis leading to blindness. Temporal arteritis: Cell composition and the possible pathogenetic role of cell-mediated immunity. Actinically degenerate elastic tissue: the prime antigen in the giant, cell (temporal) arteritis syndrome Juvenile temporal arteritis with eosinophilia: A distinct clinicopathological entity. Temporal artery biopsy is not required in all cases of suspected giant cell arteritis. Temporal artery biopsy: Is there any value in examining biopsies at multiple levels An elastic Van Gieson stain is unnecessary for the histological diagnosis of giant cell temporal arteritis. Temporal small-vessel inflammation in patients with giant cell arteritis: Clinical course and preliminary immunohistopatholigic characterization. The significance of perivascular inflammation in the absence of arteritis in temporal artery biopsy specimens. Healed or quiescent temporal arteritis versus senescent changes in temporal artery biopsy specimens. Juvenile temporal arteritis with perifollicular lymphoid proliferation resembling Kimura disease: Report of a case. Cutaneous collagenous vasculopathy with generalized telangiectasia: An immunohistochemical and ultrastructural study. Stasis dermatitis of the hand associated with an iatrogenic arteriovenous fistula. Dermatologic manifestations and management of vascular steal syndrome in hemodialysis patients with arteriovenous fistulas.
Syndromes
Additional information:
Usage: p.r.n.
Tags: nolvadex 10 mg order, discount nolvadex 10 mg visa, 10 mg nolvadex purchase overnight delivery, order 20 mg nolvadex with visa
Goran, 23 years: In all characterized cases of dyskeratosis congenita, the causative mutations are present in components of the telomerase complex.
Thordir, 56 years: Weiss H, Aledort L: Impaired platelet/connective tissue reaction in man after aspirin ingestion.