-
(786) 502-2173
-
We've gone mobile!
-
Hours: By Appointment Only
Only $0.59 per item
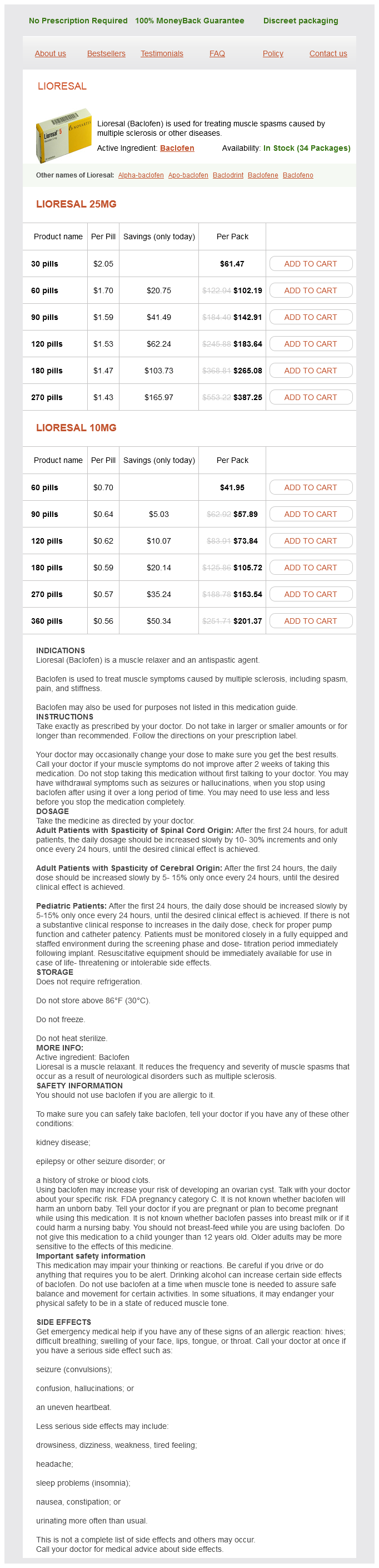
Lioresal dosages: 25 mg, 10 mg
Lioresal packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 836
Check that all four electrodes and the Dry Earth Strap are properly connected to the volunteer and the Bio Amp cable before proceeding muscle relaxant non sedating lioresal 25 mg buy otc. Before you begin Have the volunteer sit in a relaxed position, elbow bent to 90°, and the palm facing upwards. The volunteer should use his or her opposite hand to grasp the wrist of the arm from which the signal is being recorded. Add the comment: "biceps contraction" and ask the volunteer to moderately contract the biceps muscle, by trying to bend the arm further and resisting this movement with the other arm. Add the comment: "triceps contraction" and ask the volunteer to moderately contract the triceps muscle by trying to straighten out the arm and resisting this movement with the other arm. Repeat steps 12, but this time make a maximal contraction of the biceps and then the triceps muscles. In the data panel there are four channels: two for the biceps and two for the triceps. The mathematical "trick" to deal with this is to square all the values, for the square of a negative value gives you a positive one. Based on the data you collected, what can you infer is happening to the muscles as weight is added Lesson 19: Axial Skeleton Created by Aimee Williams Introduction the axial skeleton forms the vertical, central axis of the body and includes all bones of the head, neck, chest, and back and serves to protect the brain, spinal cord, heart, and lungs. The axial skeleton also serves as the attachment site for muscles that move the head, neck, and back, and for muscles that act across the shoulder and hip joints to move their corresponding limbs. Distinguish among vertebrae located in different regions of the vertebral column 3. Identify and describe unique features of a fetal skull, including fontanels, and describe their function in the fetus the axial skeleton of the adult consists of 80 bones, including the skull, the vertebral column, and the thoracic cage. The skull is formed by 22 bones and the vertebral column consists of 24 bones, each called a vertebra, plus the sacrum and coccyx. The thoracic cage includes 12 pairs of ribs in addition to the sternum, the flattened bone of the anterior chest. The rounded brain case surrounds and protects the brain and houses the middle and inner ear structures. The facial bones underlie the facial structures, form the nasal cavity, enclose the eyeballs, and support the teeth of the upper and lower jaws. In the adult, the skull consists of 22 individual bones, 21 of which are immobile and united into a single unit. The 22nd bone is the mandible (lower jaw), which is the only moveable bone of the skull. The interior space that is almost completely occupied by the brain is called the cranial cavity. The bones that form the top and sides of the brain case are usually referred to as the "flat" bones of the skull. This is a complex area that varies in depth and has numerous openings for the passage of cranial nerves, blood vessels, and the spinal cord.
Tuna Cardona (Prickly Pear Cactus). Lioresal.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96848
The left lower limb alignment also negates the potential for forward transition of body weight over the left foot during stance phase muscle spasms 6 letters generic lioresal 25 mg with visa. There is a subsequent posterior displacement of the centre of gravity in stance which produces both an associated reaction of the left upper limb into flexion and a posture of flexion/inversion within the left foot, leading to adaptive shortening of plantar structures. The secondary adaptation within the left foot further interferes with the recovery of selective postural activity in the left lower limb and trunk due to the lack of active interaction with the support surface in stance. The associated reaction to flexion within the left upper limb produces interference to gaining appropriate alignment and stability of the left scapula on the thorax which further limits the development of efficient postural activity. The lack of selective extension (weakness) within the left upper limb and repeated movement into flexion has resulted in adaptive muscle shortening. The initial clinical hypothesis, therefore, in respect of addressing the movement dysfunction would suggest the following: An improvement in distal mobility within the foot and ankle allied to increased left hip and core stability will provide a better basis for efficient weight bearing during the left stance phase of locomotion. This will be facilitated by the potential for enhanced feed-forward postural control and improved stability in stance such that there may be more efficient forward progression of the centre of gravity over the left foot. This will result in less dependence upon the walking stick for postural support and in a reduction in the associated reaction within the left arm as an involuntary response to postural instability. Refinement and testing of hypothesis through specific intervention Assessment of specific movement components with associated intervention enables further refinement and testing of the clinical hypothesis. Evaluation of outcome and further hypothesis generation Key changes in clinical presentation and the subsequent development of the clinical hypothesis is detailed below: Increased movement of the centre of gravity towards the left lower limb in stance. Improved left hip extension/abduction at the left hip with improved pelvic alignment. Walking stick is not placed as far laterally; therefore, walking with a narrower biomechanical base of support. Further hypothesis generation may relate to the extent of left shoulder girdle instability and its potential interference to further development of left hip and lower trunk stability. The improvement in postural stability and weight bearing over the left lower limb gains greater control over the associated reaction in the left upper limb. This would enable more specific assessment and evaluation of scapula stability and the potential for selective activity within the left upper limb. If it is possible to gain placement of the left upper limb to a support for hand contact. Inversion at the left ankle/foot with great toe extension and adduction resulting in poor foot contact to the plinth. This case presentation provides a brief example of the systematic decisionmaking process and the interaction between assessment and treatment. This active reasoning process will be further illustrated in subsequent chapters in relation to key aspects of functional movement.
It is the same line of pull that allows gluteus medius and gluteus medius to pull the ilium down when weight is on the limb and thus the femur cannot move spasms detoxification lioresal 25 mg purchase free shipping. The anterior portions of gluteus medius and gluteus minimus perform medial rotation of the hip because the anterior aspect of the origin attachments of these muscles are more anterior than the greater trochanter. Synergists Gluteus medius, tensor fascia latae (medially rotate the hip), and sartorius (abducts the hip) Antagonists Notable Muscle Facts the anterior section of gluteus minimus is thicker and stronger than the posterior portion. Piriformis, gemellus superior, gemellus inferior, obturator internus, obturator externus, quadratus femoris, iliopsoas, sartorius, and gluteus maximus (laterally rotate the hip); adductor magnus, adductor longus, adductor brevis, pectineus, and gracilis (adduct the hip) Implications of Shortened and/or Lengthened/ Weak Muscle Shortened: When gluteus minimus and gluteus medius are shortened, a wider stance and medial rotation of hip, as shown by toes that point inwardly, may be noted. Location Gluteus medius is located on the lateral hip, on the external surface of the ilium. Posterior ilium including iliac crest Gluteus medius Origin Insertion Origin and Insertion Origin: external surface of the lateral ilium Insertion: greater trochanter Greater trochanter Actions Gluteus minimus and gluteus medius perform the same actions: abduction and medial rotation of the hip. In addition, both gluteus minimus and gluteus medius play an important role in stabilization of the hip, particularly when one is walking. On the weight-bearing side, gluteus medius and gluteus minimus contract to pull the ilium down, so that the other ilium rises, allowing the other limb to swing through when walking. It is the same line of pull that allows gluteus minimus and gluteus medius to pull the ilium down when the weight is on the limb, and thus the femur cannot move. The anterior portion of gluteus medius and gluteus minimus perform medial rotation of the hip because the anterior aspect of the origin attachments of these muscles is more anterior than the greater trochanter. Thus, the muscles pull the greater trochanter forward, causing the femur to rotate medially. Palpation and Massage Gluteus minimis and medius can be palpated by pressing into the lateral ilium. Antagonists Piriformis, gemellus superior, gemellus inferior, obturator internus, obturator externus, quadratus femoris, iliopsoas, sartorius, and gluteus maximus (laterally rotate the hip); adductor magnus, adductor longus, adductor brevis, pectineus, and gracilis (adduct the hip) Implications of Shortened and/or Lengthened/ Weak Muscle Shortened: A shortened gluteus medius results in a wider stance, medial rotation of the hip, as shown by toes that point inwardly, and low back pain. Fascia latae refers to the broad (latae) band of fascia that surrounds all the muscles of the thigh. Thus, the lateral proximal tibia is pulled laterally, causing abduction of the hip. It can also cause the hip to be medially rotated, as indicated by toes pointing inward. Posterior ilium, iliac crest, sacrum, coccyx Gluteus maximus Origin Location Gluteus maximus is located in the superficial buttock region. Because the origin is medial to the insertion, and the muscle crosses the posterior aspect of the hip joint, a shortening of gluteus maximus pulls the gluteal tuberosity on the posterior femur posteriorly or back, thus causing lateral rotation of the hip. Gluteus maximus is also important in walking, as it contracts each time the heel strikes the ground, to halt the forward moving momentum of the trunk and upper body, thus allowing us to remain upright. This muscle contains primarily slow-twitch muscle fibers, allowing for great endurance. Outside of the quadricep group-which some consider a single muscle, gluteus maximus is the largest muscle of the body. Implications of Shortened and/or Lengthened/ Weak Muscle Shortened: Posterior tilt of the pelvis and a posture of hip lateral rotation, with toes pointed out to the side is noted.
Syndromes
Additional information:
Usage: p.c.
Tags: generic lioresal 10 mg amex, generic lioresal 10 mg mastercard, cheap lioresal 25 mg otc, buy lioresal 10 mg
Jared, 63 years: Anteriorly, the smooth surfaces of the condyles join together to form a wide groove called the patellar surface, which provides for articulation with the patella bone.
Peratur, 50 years: The first nerve, C1, emerges between the first cervical vertebra and the occipital bone.