-
(786) 502-2173
-
We've gone mobile!
-
Hours: By Appointment Only
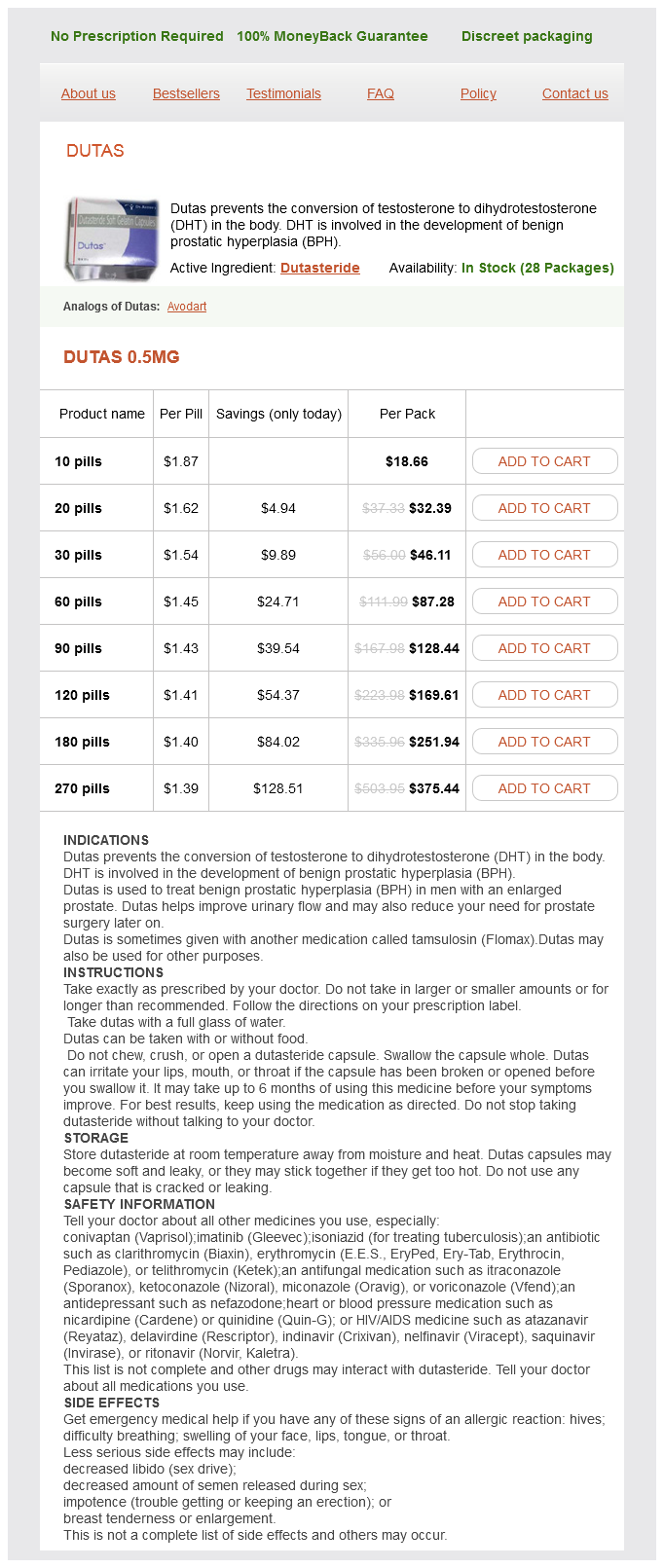
Only $1.48 per item
Dutas dosages: 0.5 mg
Dutas packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills
In stock: 670
This tongue-base obstruction leads to varying degrees of upper-airway obstruction that may complicate coordination of swallowing or adequate ventilation hair loss joint pain 0.5 mg dutas, even at rest. Initial management strategies may involve repositioning or use of an adjunctive airway device (nasal trumpet or custom oral appliance). Surgical interventions for airway and feeding concerns related to micrognathia are aimed at addressing or bypassing tongue-base obstruction. Glossopexy procedures such as tongue lip adhesion may be performed to pull the tongue forward and open the airway. For this reason, surgical gastrostomy or feeding via nasogastric tube are usually necessary to assure adequate nutritional intake. Note the site of fusion between the occlusal surfaces of the right mandible and maxilla (arrow). Distraction osteogenesis is a technique in which a bone is gradually lengthened after an initial osteotomy. During this phase (referred to as the activation phase), bone segments are separated by small increments and induction of new bone formation takes place within the gap. After the desired lengthening has been achieved, a consolidation period ensues in which the bone segments are held securely in their advanced position. The immature bone (referred to as "the regenerate" bone) remodels and matures during this six week time frame, after which the distraction hardware is removed. Since distraction proceeds at a slow pace, related muscles, blood vessels, nerves, skin, and mucosa are also elongated during the process. The first reported use of mandibular distraction in children with micrognathia was in 1992. As part of this mandibular deformity, these infants lack a well defined glenoid fossa on the affected side. Therefore, if mandibular distraction is performed, the posterior mandibular segment may not engage properly against the skull base. This lack of engagement allows seemingly infinite posterior movement of the posterior mandibular segment into the soft tissue of the mastoid area, thus preventing effective anterior advancement of the mandible with distraction of the mobile segments. If inadequate growth is observed, the jaw may be advanced through distraction of the grafted rib segment. In children with unilateral mandibular hypoplasia, unilateral mandibular distraction is an option. The indications for this technique are based on malocclusion and facial asymmetry, so surgical intervention is typically deferred until later in childhood, even in patients in whom costal cartilage grafting is not necessary. Free-tissue transfer with a fibular free flap reconstruction provides the largest amount of available vascularized bone stock and is especially useful in patients with severe hypoplasia in whom a free bone graft is neither practical nor advisable.
Amukkirag (Ashwagandha). Dutas.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96916
As the fusion proceeds posteriorly hair loss 4 months after baby dutas 0.5 mg with visa, the nasal septum grows down to merge with the cephalic aspect (maxillary crest) of the newly formed palate. The secondary palate receives innervation and blood supply from the greater and lesser palatine vessels. Disorders of neural crest cell development and disruption of crest migration are the source of many congenital malformations involving the mandible and maxilla. It is also referred to as Goldenhar syndrome in severe cases or as craniofacial microsomia (previously termed hemifacial microsomia) in milder forms. The pattern of malformation typically involves the maxillary, temporal, and zygomatic bones, which are classically small and flat. Other findings may include microtia, aural atresia, ocular tumors (epibulbar dermoids), cleft lip and palate, lateral facial cleft (macrostomia), vertebral anomalies (hemivertebrae, spina bifida), and cardiac abnormalities. The cause is unknown, but given the pattern of malformations, a disorder of neural crest cell development could be implicated. In cases of isolated hemifacial microsomia, an ischemia hypothesis affecting the distribution of either the first aortic arch (maxillary) artery or the second aortic arch (stapedial) artery has also been proposed. Typically, this disorder presents in association with limb abnormalities and is grouped as the hypoglossia-hypodactylia syndrome. Although a conclusive cause for microglossia remains unknown, several theories have been postulated. Certain medications used during pregnancy such as diazepam, chlorpromazine, meclizine and trimethobenzamide have been thought to possibly contribute to the condition. Interference of the second aortic arch (stapedial artery) blood supply has also been postulated as a potential cause leading to hypoplasia of the anterior part of the tongue. Gastrostomy placement for feeding support as well as early mandibular distraction osteogenesis during infancy have been described for initial management of microglossia and glossoptosis. Pierre Robin sequence is a triad of micrognathia, glossoptosis, and u-shaped cleft palate that occurs in approximately 1 in 8,500 births. Various hypotheses exist in regards to genetic or environmental factors, but the underlying cause in each case is related to underdevelopment of the mandible. In cases of oligohydramnios, mandibular hypoplasia may occur as a result of hyperflexion of the neck, compressing the chin against the chest. Incomplete clefting of the secondary palate occurs as posterior positioning of the tongue mechanically prevents complete fusion of the palatine shelves. Such glossoptosis may cause clefting of the secondary palate as posterior positioning of the tongue can interfere with normal fusion of the palatine shelves, a syndromic form of Robin sequence. The mandibular hypoplasia may involve the body, ramus, coronoid, and/or condylar processes. The temporomandibular joints themselves may be malformed, limiting function and complicating subsequent mandibular reconstruction. This syndrome may occur along a wide spectrum from mild to severe phenotypes, even within similarly afflicted family members.
Adenoidectomy is indicated for recurrent or chronic adenoiditis that is refractory to antimicrobial agents hair loss icd 9 cheap 0.5 mg dutas visa. Adenoidectomy is effective to reduce infections from both adenoiditis and sinusitis and may be considered as a surgical option prior to endoscopic sinus surgery. Patients who do not respond to adenoidectomy may still require endoscopic sinus surgery. Histologic examination of adenoid tissue is required for definition of the clinical issue. In particular, children battling cancer are at greater risk for many of the infectious diseases discussed in this chapter. Children undergoing oncologic therapies are at risk for mucositis that can severely affect their already diminished quality of life. The mucositis is important in that it removes a layer of protection, further potentiating the risk for viral, fungal, or bacterial infection of the oral cavity, which can easily become systemic infections in these individuals. Furthermore, xerostomia can occur, removing salivary defense mechanisms and increasing the risk of dental caries and odontogenic infections. Recognizing these limitations of the immune system and innate defenses of children undergoing oncologic treatments will allow careful consideration in the workup and treatment recommendations offered to this subset of patients. Note normal filling of jugular vein, sigmoid sinus, and transverse sinus on right (arrow) with absence of filling of the same venous structures on left. Treatment includes beta-lactamase stable antibiotics, penicillin plus metronidazole, or clindamycin for three to six weeks or longer. Associated peritonsillar or parapharyngeal spaces abscesses, if present, require drainage. Although asymmetric tonsillar size may represent malignancy such as lymphoma, the incidence of malignancy in otherwise asymptomatic children without constitutional signs and symptoms is low. Recurrent or chronic pharyngitis can also be caused by supraesophageal reflux of gastric contents. Acidic gastric contents contain pepsin and food materials, both of which are irritating to pharyngeal mucosa. Prevalence of human papillomavirus in the oral cavity/oropharynx in a large population of children and adolescents. Oral manifestations in human immunodeficiency virus infected children in highly active antiretroviral therapy era. Oral manifestations of inflammatory bowel disease: a review based on the observation of six cases. Colchicine prophylaxis for frequent periodic fever, aphthous stomatitis, pharyngitis and adenitis episodes. A randomized controlled trial of tonsillectomy in periodic fever, aphthous stomatitis, pharyngitis, and adenitis syndrome. Tonsillectomy in children with periodic fever with aphthous stomatitis, pharyngitis, and adenitis syndrome. Hospitalizations for Kawasaki syndrome among children in the United States, 1997-2007.
Syndromes
Additional information:
Usage: a.c.
Tags: purchase dutas 0.5 mg on line, dutas 0.5 mg order without a prescription, 0.5 mg dutas order overnight delivery, buy 0.5 mg dutas visa
Pedar, 60 years: In rare cases, vessels can be found in or near the vicinity of the cephalocele sac. In addition, the exudates in these patients may be harder to clear both due to increased viscosity and mucociliary dysfunction. In revision ethmoid surgery, the skull base must be identified early, and the lateral cavity should be examined for undissected cells.
Vatras, 30 years: Sleep-related breathing disorder in Duchenne muscular dystrophy: disease spectrum in the paediatric population. This adipose tissue is much smaller than the malar fat pad, but its elevation or increased volume can significantly improve results in midface rejuvenation. Topical mitomycin application after laryngotracheal reconstruction: a randomized, double-blind, placebo-controlled trial.
Osmund, 62 years: A study in 1982 did demonstrate some benefit in nonallergic rhinitis patients when first-generation antihistamines and decongestants were combined. All surgeons who perform rhytidectomy should preoperatively inform their patients of the potential risks, including hematoma, infection, skin flap necrosis, nerve injury, poor scarring, alopecia, etc. Branches from the maxillary division of the trigeminal, facial, glossopharyngeal, and vagus nerves pro vide sensory innervation.
Giores, 40 years: They again utilize the intrinsic curvature and spring of conchal cartilage to reconstruct the collapsed middle vault. Montelukast is the only leukotriene modifier that has been approved in the United States to be used for the symptoms of seasonal and perennial allergic rhinitis. Symptoms are present at birth with excessive secretions, respiratory difficulties, feeding difficulties and aspiration.
Sanford, 35 years: The fossa of Rosenmuller, torus tubarius, and the orifice of the eustachian canal are on the lateral wall of the nasopharynx. Although these tissues possess major aesthetic roles, the eyelids first and foremost serve a functional role to protect and nurture the eye. Note that the plane of the true ostium is tilted axially as compared to the sagitally-oriented surgical antrostomy.
Kaelin, 46 years: Evidence of vestibular and balance dysfunction in children with profound sensorineural hearing loss using cochlear implants. An adult suffering from acute supraglottitis may appear ill with restlessness and accessory respiratory muscle use with intercostal or suprasternal retractions. The dermis is deep to the epidermis and is tightly adherent to it as a result of its irregular border.
Daro, 53 years: Again, pain that is disproportionate to the procedure is the most common presenting complaint. Acoustic rhinometry predicts tolerance of nasal continuous positive airway pressure: A pilot study. Patients with thick sebaceous skin have a higher risk of developing flap necrosis, trapdoor deformity, and depressed scars.